

Kidney outcomes of malignant hypertension-associated thrombotic microangiopathy in patients with and without IgA nephropathy: a propensity score-matched analysis
- PMID: 40104549
- PMCID: PMC11914877
- DOI: 10.1093/ckj/sfaf017
Kidney outcomes of malignant hypertension-associated thrombotic microangiopathy in patients with and without IgA nephropathy: a propensity score-matched analysis
Abstract
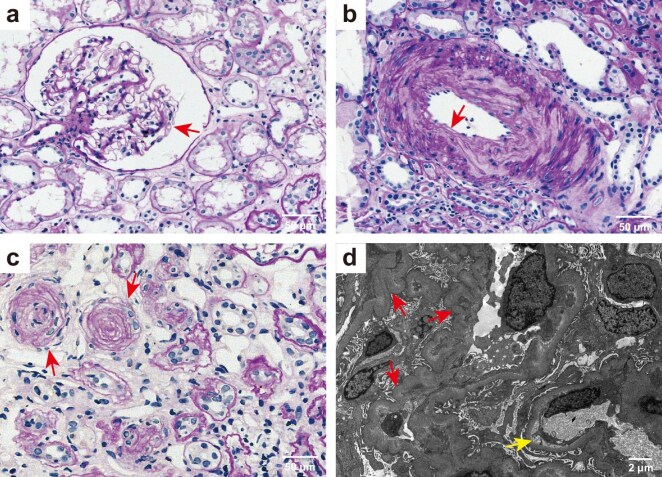
Background: IgA nephropathy (IgAN) can cause hypertension, and severe hypertension can exacerbate the progression of IgAN. However, the long-term kidney outcome of malignant hypertension (mHTN)-associated thrombotic microangiopathy (TMA) with IgAN is not well defined.
Methods: A total of 292 individuals with mHTN-associated TMA confirmed by kidney biopsy were included. Propensity score matching (PSM) analysis was performed to adjust for clinical characteristics in the comparison between cases with and without IgAN. Cox regression analysis was utilized to identify risk factors associated with long-term kidney outcome.
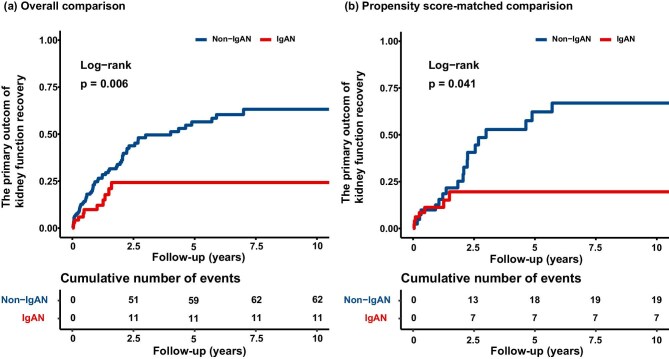
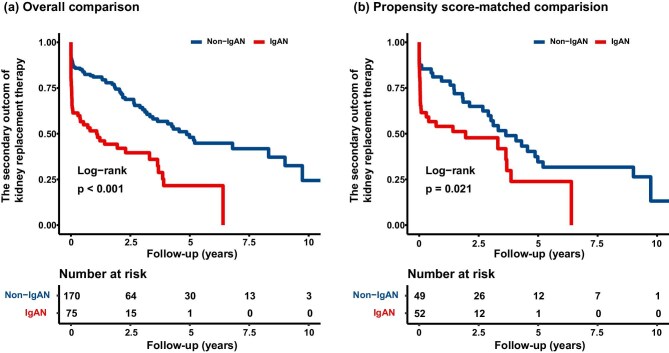
Results: A total of 86 mHTN-associated TMA with IgAN patients were compared with 206 mHTN-associated TMA with non-IgAN patients. After PSM, 61 pairs of patients with mHTN-associated TMA were matched. The mHTN-associated TMA with IgAN patients exhibited significantly lower serum albumin, higher 24-hour proteinuria, and a higher ratio of global sclerosis than those with non-IgAN. mHTN-associated TMA with IgAN was independently associated with impaired kidney function recovery [hazard ratio (HR), 0.48; 95% confidence interval (CI), 0.24-0.96, P = .038] compared with non-IgAN. This association remained significant after PSM (HR, 0.41; 95% CI, 0.17-0.99, P = .047). In addition, mHTN-associated TMA with IgAN was independently associated with kidney replacement therapy (KRT) compared with non-IgAN (HR, 2.31; 95% CI, 1.38-3.88; P = .002). This difference remained significant after PSM comparison (HR, 2.38; 95%CI, 1.14-4.99; P = .021). In addition, mHTN-associated TMA with IgAN patients had a higher incidence of receiving KRT and a lower incidence of kidney function recovery with a 25% reduction in creatinine levels than in non-IgAN patients, regardless of intensive blood pressure control.
Conclusions: The long-term kidney outcomes for mHTN-associated TMA patients with concomitant IgAN are significantly poorer than that of patients with non-IgAN. Monitoring kidney pathological characteristics will aid management and risk assessment at an early stage.
Keywords: IgA nephropathy; kidney biopsy; kidney replacement therapy; malignant hypertension; thrombotic microangiopathy.
© The Author(s) 2025. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Glomerular Hematuria as a Predictor of Renal Prognosis in Malignant Hypertension Patients with Thrombotic Microangiopathy: A Propensity Score-Matched Analysis of a Biopsy-Based Cohort Study.Kidney Dis (Basel). 2024 Sep 12;10(6):479-491. doi: 10.1159/000541332. eCollection 2024 Dec. Kidney Dis (Basel). 2024. PMID: 39664331 Free PMC article.
-
Thrombotic microangiopathy in patients with malignant hypertension.Nephrol Dial Transplant. 2023 May 4;38(5):1217-1226. doi: 10.1093/ndt/gfac248. Nephrol Dial Transplant. 2023. PMID: 36002030
-
Kidney Outcomes Following Angiotensin Receptor-Neprilysin Inhibitor vs Angiotensin-Converting Enzyme Inhibitor/Angiotensin Receptor Blocker Therapy for Thrombotic Microangiopathy.JAMA Netw Open. 2024 Sep 3;7(9):e2432862. doi: 10.1001/jamanetworkopen.2024.32862. JAMA Netw Open. 2024. PMID: 39264627 Free PMC article.
-
Glomerular endothelial activation, C4d deposits and microangiopathy in immunoglobulin A nephropathy.Nephrol Dial Transplant. 2021 Mar 29;36(4):581-586. doi: 10.1093/ndt/gfz241. Nephrol Dial Transplant. 2021. PMID: 31755918 Review.
-
Non-immunosuppressive treatment for IgA nephropathy.Cochrane Database Syst Rev. 2024 Feb 1;2(2):CD003962. doi: 10.1002/14651858.CD003962.pub3. Cochrane Database Syst Rev. 2024. PMID: 38299639 Free PMC article.
References
-
- Sevillano ÁM, Cabrera J, Gutiérrez E et al. Malignant hypertension: a type of IgA nephropathy manifestation with poor prognosis. Nefrol Publ Soc Espanola Nefrol 2015;35:42–49. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
