

[Risk factors and development of a prediction model of enteral feeding intolerance in critically ill children]
- PMID: 40105078
- PMCID: PMC11928032
- DOI: 10.7499/j.issn.1008-8830.2409102
[Risk factors and development of a prediction model of enteral feeding intolerance in critically ill children]
Abstract
Objectives: To explore the risk factors of feeding intolerance (FI) in critically ill children receiving enteral nutrition (EN) and to construct a prediction nomogram model for FI.
Methods: A retrospective study was conducted to collect data from critically ill children admitted to the Pediatric Intensive Care Unit of Xiangya Hospital, Central South University, between January 2015 and October 2020. The children were randomly divided into a training set (346 cases) and a validation set (147 cases). The training set was further divided into a tolerance group (216 cases) and an intolerance group (130 cases). Multivariate logistic regression analysis was used to screen for risk factors for FI in critically ill children receiving EN. A nomogram was constructed using R language, which was then validated on the validation set. The model's discrimination, calibration, and clinical net benefit were evaluated using receiver operating characteristic curves, calibration curves, and decision curves.
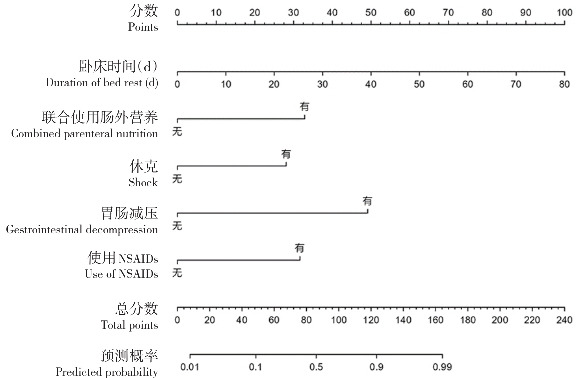
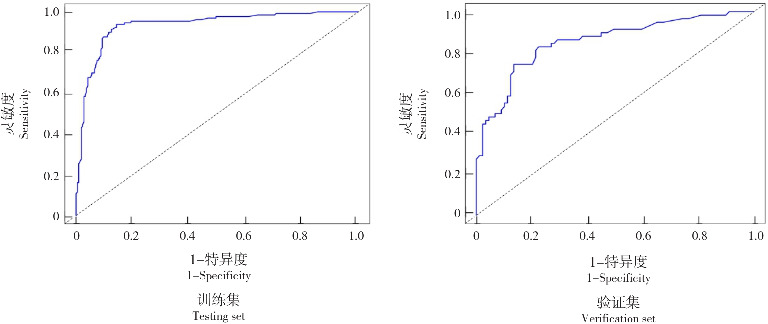
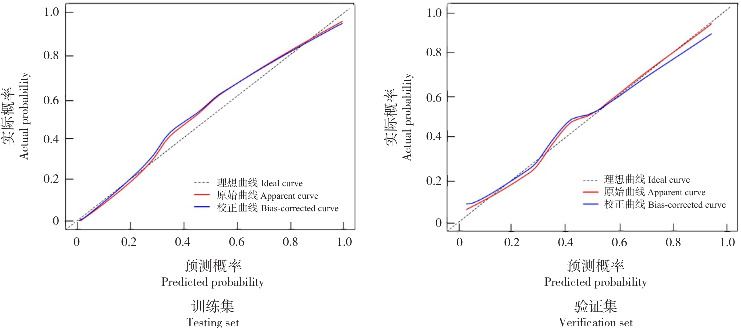
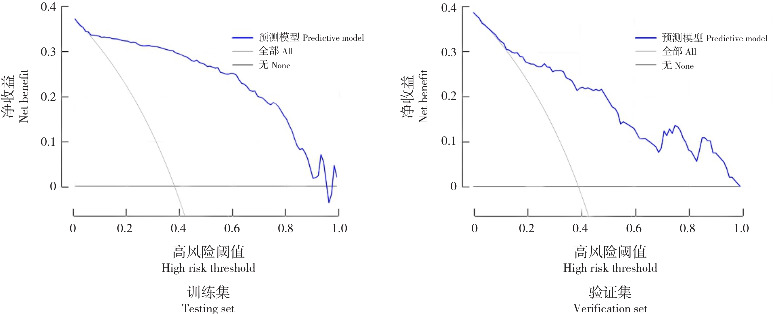
Results: Duration of bed rest, shock, gastrointestinal decompression, use of non-steroidal anti-inflammatory drugs, and combined parenteral nutrition were identified as independent risk factors for FI in critically ill children receiving EN (P<0.05). Based on these factors, a nomogram prediction model for FI in critically ill children receiving EN was developed. The area under the receiver operating characteristic curve for the training set and validation set was 0.934 (95%CI: 0.906-0.963) and 0.852 (95%CI: 0.787-0.917), respectively, indicating good discrimination of the model. The Hosmer-Lemeshow goodness-of-fit test showed that the model had a good fit (χ 2=12.559, P=0.128). Calibration curve and decision curve analyses suggested that the model has high predictive efficacy and clinical application value.
Conclusions: Duration of bed rest, shock, gastrointestinal decompression, use of non-steroidal anti-inflammatory drugs, and combined parenteral nutrition are independent risk factors for FI in critically ill children receiving EN. The nomogram model developed based on these factors exhibits high predictive efficacy and clinical application value.
目的: 探讨危重患儿肠内营养(enteral nutrition, EN)发生喂养不耐受(feeding intolerance, FI)的危险因素,并构建列线图模型。方法: 回顾性收集2015年1月—2020年10月中南大学湘雅医院儿童重症监护室收治的危重患儿资料,随机分为训练集组(346例)和验证集组(147例)。训练集组进一步分为耐受组(216例)和不耐受组(130例)。采用多因素logistic回归分析筛选危重患儿EN发生FI的危险因素,利用R语言构建列线图,对验证集组进行验证。分别采用受试者操作特征曲线、校准曲线和决策曲线分析评价模型的区分度、校准度和临床净收益。结果: 卧床时间、休克、胃肠减压、使用非甾体类抗炎药、联合使用肠外营养是危重患儿EN发生FI的独立危险因素 (P<0.05)。基于这些因素构建EN危重患儿发生FI的列线图预测模型,受试者操作特征曲线分析结果显示,训练集组和验证集组曲线下面积分别为0.934(95%CI:0.906~0.963)和0.852(95%CI:0.787~0.917),表明模型的区分度良好。Hosmer-Lemeshow拟合优度检验表明该模型拟合度良好( χ 2=12.559,P=0.128)。校准曲线分析和决策曲线分析提示该模型的预测效能和临床应用价值较高。结论: 卧床时间、休克、胃肠减压、使用非甾体类抗炎药物和联合使用肠外营养是危重患儿EN发生FI的独立危险因素;根据这些因素构建的列线图模型有较高的预测效能和临床应用价值。.
Keywords: Child; Enteral nutrition; Feeding intolerance; Nomogram; Prediction model; Risk factor.
Conflict of interest statement
所有作者均声明不存在利益冲突。
Figures
References
-
- 纪健, 钱素云. 2017版 美国危重患儿营养支持治疗实施与评价指南解读[J]. 中华儿科杂志, 2018, 56(5): 332-335. DOI: 10.3760/cma.j.issn.0578-1310.2018.05.005. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials