

Biventricular vs. right ventricular pacing devices in patients anticipated to require frequent ventricular pacing (BioPace)
- PMID: 40105785
- PMCID: PMC11921422
- DOI: 10.1093/europace/euaf029
Biventricular vs. right ventricular pacing devices in patients anticipated to require frequent ventricular pacing (BioPace)
Erratum in
-
Correction to: Biventricular vs. right ventricular pacing devices in patients anticipated to require frequent ventricular pacing (BioPace).Europace. 2025 Oct 7;27(10):euaf253. doi: 10.1093/europace/euaf253. Europace. 2025. PMID: 41066377 Free PMC article. No abstract available.
Abstract
Aims: Right ventricular (RV) pacing may promote left ventricular (LV) dysfunction. Particularly in patients with preserved LV ejection fraction (LVEF), narrow QRS, and anticipated high ventricular pacing burden (HVPB), evidence is missing that biventricular (BiV) pacing can improve clinical outcome. We therefore evaluated whether implantation of a BiV pacing device (BiVPD) compared with a RV pacing device (RVPD) may improve clinical outcome in predominantly this kind of patients.
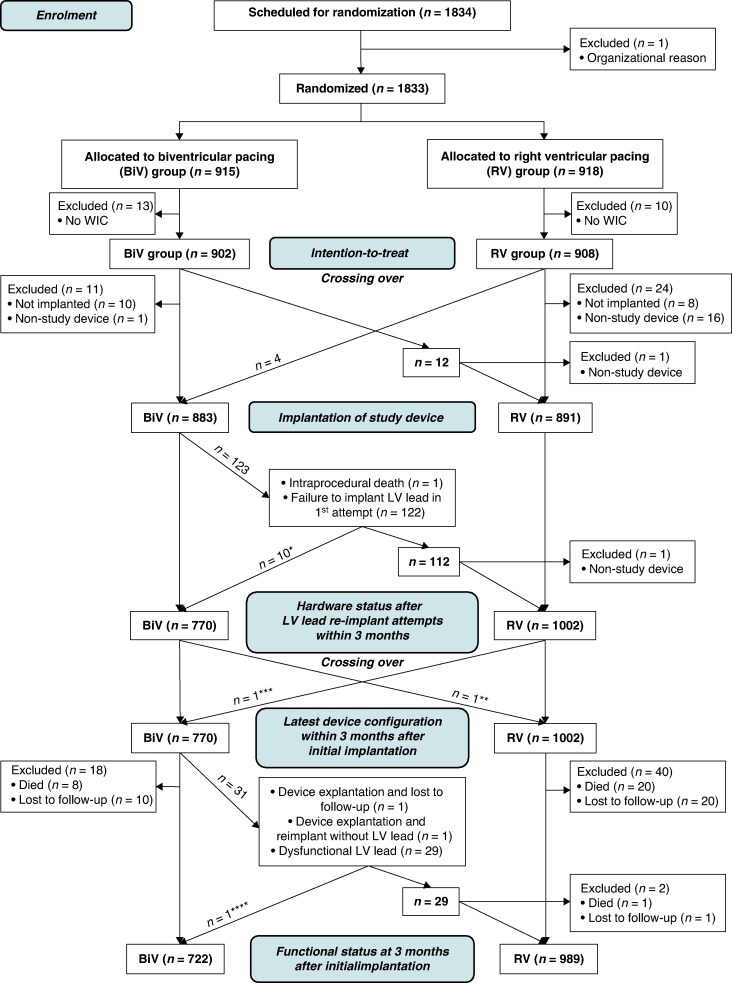
Methods and results: In the Biventricular Pacing for atrioventricular Block to Prevent Cardiac Desynchronization (BioPace) trial [multicentre, single-blinded (patients), randomized, parallel group], patients were equally allocated to either receive a BiVPD or a RVPD. Co-primary endpoints were (i) the composite of time to death or first heart failure hospitalization and (ii) survival time. We analysed 1810 randomized patients (median age: 73.5 years; female sex: 31.7%; mean LVEF 55.4%; mean QRS 118.4 ms), 902 to BiV and 908 to RV pacing. During mean follow-up of 68.8 months, the difference in the primary composite endpoint between both groups [346 vs. 363 events, hazard ratio (HR) 0.878; 95% confidence interval (CI) 0.756-1.020; P = 0.0882) or in mortality (305 vs. 307 deaths, HR 0.926; 95% CI 0.789-1.088; P = 0.3492) was smaller than 20%.
Conclusion: In patients, predominantly with preserved LVEF, narrow QRS, and HVPB, superiority of implanting BiVPDs compared with RVPDs could not be proven. Right ventricular pacing may be less harmful for this kind of patients than often suggested and primary BiV pacing does not clearly improve their clinical outcome.
Clinical trial registration: Registered in ClinicalTrials.gov, number NCT00187278 (https://clinicaltrials.gov/ct2/show/study/NCT00187278).
Keywords: Biventricular pacing; Cardiac pacing; Heart failure; Mortality; Pacing-induced cardiomyopathy; Right ventricular pacing.
© The Author(s) 2025. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: R.C.F. received consultancy/lecture fees and refunding of travel cost/congress registration fees from Abbott CRM with respect of the conduct of the study. H.-H.M. received refunding of travel costs from Abbott with respect of the conduct of the study. M.L. received grants and consultancy/lecture fees from Abbott. M.D.C. received personal fees from Abbott. M.W. received grants and personal fees from Abbott with respect to the conduct of the study. G.H. received research grants through the Heart Center Leipzig from Abbott.
Figures


References
-
- Glikson M, Nielsen JC, Kronborg MB, Michowitz Y, Auricchio A, Barbash IM et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J 2021;42:3427–520. - PubMed
-
- Barold SS. Adverse effects of ventricular desynchronization induced by long-term right ventricular pacing. J Am Coll Cardiol 2003;42:624–6. - PubMed
-
- Wilkoff BL, Cook JR, Epstein AE, Greene HL, Hallstrom AP, Hsia H et al. Dual-chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: the Dual Chamber and VVI Implantable Defibrillator (DAVID) trial. JAMA 2002;288:3115–23. - PubMed
-
- Sweeney MO, Hellkamp AS, Ellenbogen KA, Greenspon AJ, Freedman RA, Lee KL et al. Adverse effect of ventricular pacing on heart failure and atrial fibrillation among patients with normal baseline QRS duration in a clinical trial of pacemaker therapy for sinus node dysfunction. Circulation 2003;107:2932–7. - PubMed
-
- Kiehl EL, Makki T, Kumar R, Gumber D, Kwon DH, Rickard JW et al. Incidence and predictors of right ventricular pacing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm 2016;13:2272–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
