

The efficacy of islet autoantibody screening with or without genetic pre-screening strategies for the identification of presymptomatic type 1 diabetes
- PMID: 40105972
- PMCID: PMC12069122
- DOI: 10.1007/s00125-025-06408-4
The efficacy of islet autoantibody screening with or without genetic pre-screening strategies for the identification of presymptomatic type 1 diabetes
Abstract
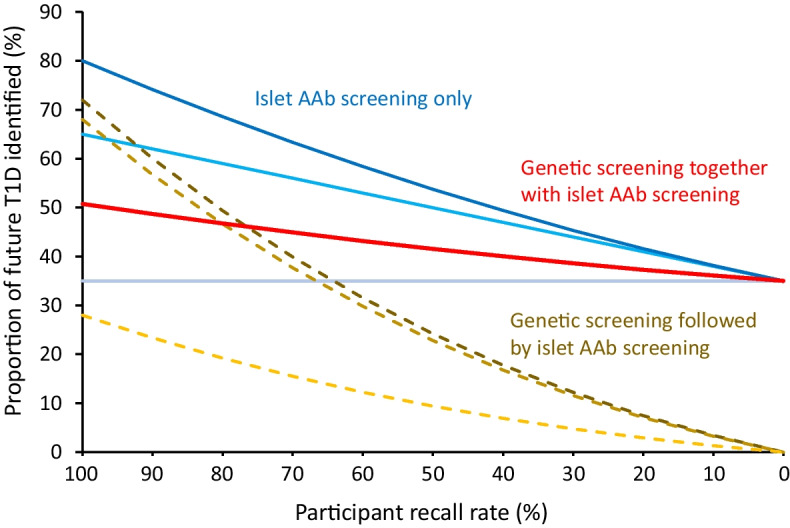
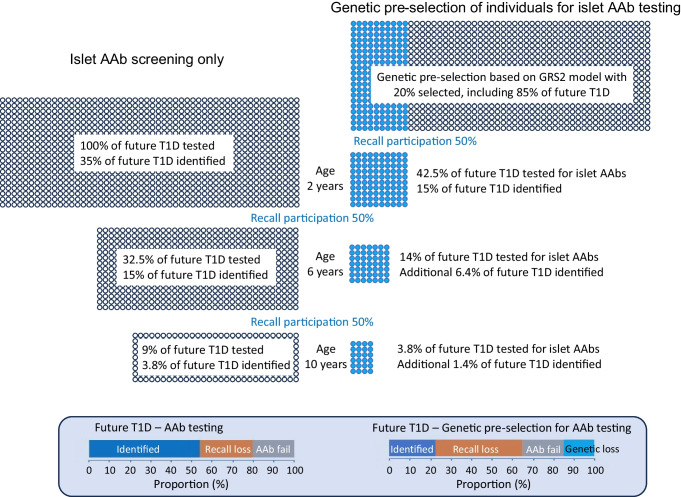
Early detection of type 1 diabetes, in its presymptomatic stage, offers significant clinical advantages, including treatment that can delay disease onset. Current screening focuses on identifying islet autoantibody positivity, with proposed optimal testing at ages 2, 6 and 10 years potentially achieving up to 80% sensitivity. However, challenges arise from participation rates and costs associated with multiple screenings. Genetic pre-screening has been suggested as a complementary strategy to target high-risk individuals prior to autoantibody testing, but its real-world benefits remain uncertain. Broad genetic selection strategies, based on family history, HLA typing or polygenic risk scores, can identify subsets of the population at elevated risk. However, these approaches face issues like low recall rates, socioeconomic biases and limited applicability across diverse ancestries. Additionally, the cost-effectiveness and infrastructure requirements of integrating genetic testing into routine healthcare remain significant hurdles. The combined use of genetic and autoantibody testing could improve predictive value, especially with innovations like point-of-care genetic testing. Yet, the ultimate success of any screening programme depends less on specific strategies and more on maximising public and healthcare-provider engagement, ensuring high participation, and addressing socioeconomic and demographic disparities. Digital-health infrastructure may play a crucial role in improving recall rates and maintaining follow-up adherence. In conclusion, while repeated islet autoantibody screening remains the most effective standalone approach, conducting genetic screening prior to islet autoantibody testing may be practical in certain contexts, provided that sufficient resources and equitable strategies are employed. Public engagement and robust infrastructure are essential to realising the full potential of early type 1 diabetes detection programmes.
© 2025. The Author(s).
Conflict of interest statement
Funding: Open Access funding enabled and organized by Projekt DEAL. This work was supported by The Leona M. and Harry B. Helmsley Charitable Trust (Helmsley) grant G-2103-05036 and the German Federal Ministry of Education and Research (grant reference: FZK 01KX1818). EB, GG, MK, OK, VL, PN, FP, ZS, AS and A-GZ are part of EDENT1FI, which is supported by the Innovative Health Initiative Joint Undertaking (IHI JU) under grant agreement no. 101132379. This JU receives support from the European Union’s Horizon Europe research and innovation programme, The Leona M. and Harry B. Helmsley Charitable Trust, Breakthrough T1D, EFPIA, COCIR, Vaccines Europe, EuropaBio and MedTech. Additional funding is provided to associated UK partners through the UK Research and Innovation (UKRI) Guarantee Fund. Disclaimer: Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the aforementioned funding partners and cannot be held responsible for them. Authors’ relationships and activities: All authors declare that there are no relationships or activities that might bias, or be perceived to bias, their work. Contribution statement: This manuscript is a result of discussion among all authors of the article and who conducted screening in the EDENT1FI consortium. EB and A-GZ drafted the manuscript. All authors have reviewed and approved the content of the article.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
