

Safety and efficacy of SGLT2 inhibitors in heart failure patients with ischemic and non-ischemic etiologies: a systematic review and meta-analyses
- PMID: 40106055
- PMCID: PMC11923348
- DOI: 10.1186/s43044-025-00623-5
Safety and efficacy of SGLT2 inhibitors in heart failure patients with ischemic and non-ischemic etiologies: a systematic review and meta-analyses
Abstract
Background: Sodium-glucose cotransporter 2 inhibitors (SGLT2is) show promise as a therapy for heart failure (HF); however, the safety and efficacy of SGLT2i in different HF etiologies are uncertain, thus arising the need for a meta-analyses.
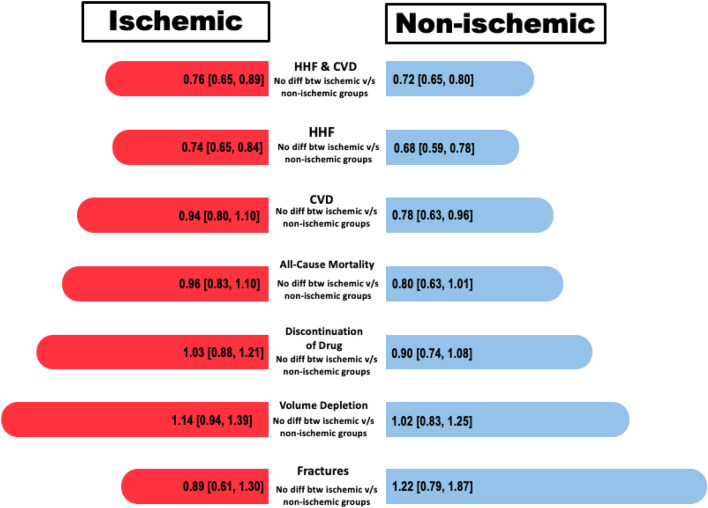
Main text: PubMed and Scopus were queried until May 2023 for studies comparing SGLT2i with placebo in HF patients with ischemic and non-ischemic etiologies. Meta-analyses were performed using risk ratio and hazard ratio. A fixed effect model was used. Outcomes assessed were hospitalization due to HF (HHF), cardiovascular death (CVD), CVD/HHF, all-cause mortality, volume depletion, fracture, and discontinuation of drug due to adverse effects. Four RCTs were included (15,676 patients). Analysis revealed no significant differences in CVD/HHF between ischemic [HR: 0.77 (0.70-0.86) P < 0.00001] and non-ischemic patients [HR: 0.72 (0.65-0.80) P < 0.00001] using SGLT2i (P = 0.35). Significant reductions were seen in HHF in both ischemic [RR 0.74 (0.65-0.84) P < 0.00001] and non-ischemic [RR 0.68 (0.59-0.78) P < 0.00001] patients (P = 0.39), with the effect more notable in the non-ischemic cohort. However, CVD significantly decreased in non-ischemic patients [RR 0.78 (0.63-0.95) P = 0.01], whereas no significant reduction was noted in ischemic patients [RR 0.94 (0.80-1.10) P = 0.43] (P-interaction = 0.15). All-cause mortality was significantly reduced in non-ischemic patients [RR 0.80 (0.67-0.96) P = 0.02] but not in ischemic patients [RR 0.96 (0.83-1.10) P = 0.52]. No significant safety events were observed in the SGLT2i cohort including volume depletion [RR 1.08 (0.94-1.25) P = 0.26], fracture [RR 1.02 (0.77-1.36) P = 0.88], or discontinuation of drug due to adverse effects [RR 0.97 (0.86-1.10) P = 0.65].
Conclusion: Similar CVD/HHF outcomes for ischemic and non-ischemic patients with SGLT2i. Significant HHF reductions in both groups. Non-ischemic patients showed greater improvements in CVD and all-cause mortality. However, no subgroup difference between ischemic and non-ischemic cause of heart failure was noted in our analysis.
Keywords: All-cause mortality; Cardiovascular death; Heart failure; Hospitalization due to heart failure; Meta-analyses; Sodium-glucose cotransporter 2 inhibitors.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate.: Not applicable. Consent for publication: Not applicable. Competing interest: The authors declared that they have no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures










References
-
- Bergethon KE, Ju C, DeVore AD, Hardy NC, Fonarow GC, Yancy CW, Heidenreich PA, Bhatt DL, Peterson ED, Hernandez AF (2016) Trends in 30-day readmission rates for patients hospitalized with heart failure: findings from the get with the guidelines-heart failure registry. Circ Heart Fail 9:1. 10.1161/CIRCHEARTFAILURE.115.002594e002594 - PMC - PubMed
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators (2018) Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990−2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392:1789–1858 - PMC - PubMed
-
- Adamo M, Gardner RS, McDonagh TA, Metra M (2022) The “Ten Commandments” of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 43(6):440–441. 10.1093/eurheartj/ehab853 - PubMed
-
- Neal B, Perkovic V, Mahaffey KW et al (2017) Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 377:644–657 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous