

Optimising fluid therapy during venoarterial extracorporeal membrane oxygenation: current evidence and future directions
- PMID: 40106084
- PMCID: PMC11923310
- DOI: 10.1186/s13613-025-01458-8
Optimising fluid therapy during venoarterial extracorporeal membrane oxygenation: current evidence and future directions
Abstract
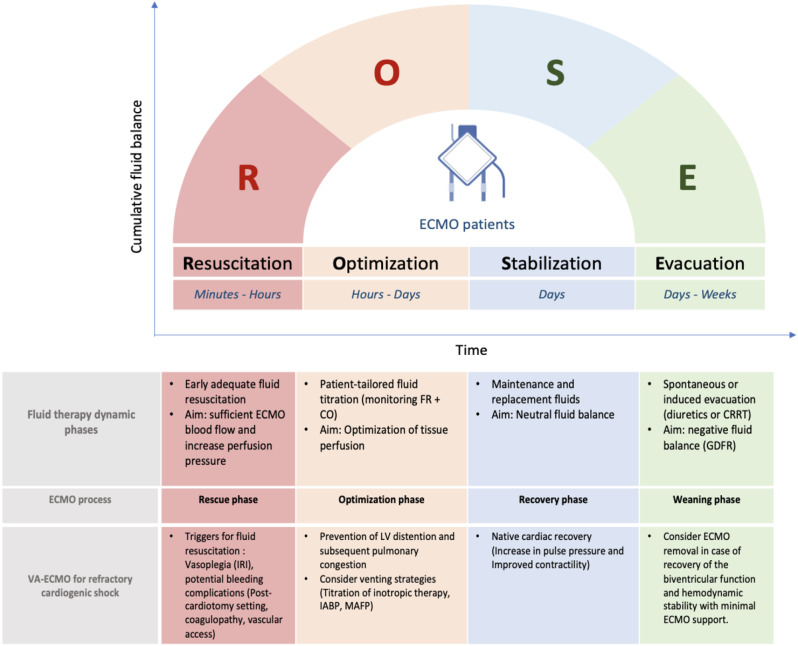
Venoarterial extracorporeal membrane oxygenation (VA-ECMO) offers an immediate and effective mechanical cardio-circulatory support for critically ill patients with refractory cardiogenic shock or selected refractory cardiac arrest. As fluid therapy is routinely performed as a component of initial hemodynamic resuscitation of ECMO supported patients, this narrative review intends to summarize the rationale and the evidence on the fluid resuscitation strategy in terms of fluid type and dosing, the impact of fluid balance on outcomes and fluid responsiveness assessment in VA-ECMO patients. Several observational studies have shown a deleterious impact of positive fluid balance on survival and renal outcomes. With regard to the type of crystalloids, further studies are needed to evaluate the safety and efficacy of saline versus balanced solutions in terms of hemodynamic stability, renal outcomes and survival in VA-ECMO setting. The place and the impact of albumin replacement, as a second-line option, should be investigated. During VA-ECMO run, the fluid management approach could be divided into four phases: rescue or salvage, optimization, stabilization, and evacuation or de-escalation. Echocardiographic assessment of stroke volume changes following a fluid challenge or provocative tests is the most used tool in clinical practice to predict fluid responsiveness. This review underscores the need for high-quality evidence regarding the optimal fluid strategy and the choice of fluid type in ECMO supported patients. Pending specific data, fluid therapy needs to be personalized and guided by dynamic hemodynamic approach coupled to close monitoring of daily weight and fluid balance in order to provide adequate ECMO flow and tissue perfusion while avoiding harmful effects of fluid overload.
Keywords: Critically ill patients; Extracorporeal membrane oxygenation; Fluid management; Fluid responsiveness.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: Not required. Consent for publication: On behalf of all authors, the corresponding author provides consent for the publication of the manuscript detailed above, including any accompanying images or data contained within the manuscript that may directly or indirectly disclose the authors’ identity. Competing interests: The authors have no potential conflicts of interest to declare.
Figures
References
-
- Mongardon N, De Roux Q, Clariot S. Veno-arterial ECMO in critically ill patients: the age of maturity? Anaesth Crit Care Pain Med. 2018;37(3):193–4. - PubMed
-
- Théroux P, Armstrong PW, Mahaffey KW, et al. Prognostic significance of blood markers of inflammation in patients with ST-segment elevation myocardial infarction undergoing primary angioplasty and effects of Pexelizumab, a C5 inhibitor: a substudy of the COMMA trial. Eur Heart J. 2005;26(19):1964–70. - PubMed
-
- Frydland M, Ostrowski SR, Møller JE, et al. Plasma concentration of biomarkers reflecting endothelial Cell- and glycocalyx damage are increased in patients with suspected ST-Elevation myocardial infarction complicated by cardiogenic shock. Shock. 2018;50(5):538–44. - PubMed
-
- Kohsaka S, Menon V, Lowe AM, et al. Systemic inflammatory response syndrome after acute myocardial infarction complicated by cardiogenic shock. Arch Intern Med. 2005;165(14):1643–50. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
