

Healthcare Expenditure Trajectories in the Last 5 Years of Life: A Retrospective Cohort Study of Decedents with Advanced Cancer and End-Stage Organ Diseases
- PMID: 40106134
- PMCID: PMC12209486
- DOI: 10.1007/s41669-025-00573-3
Healthcare Expenditure Trajectories in the Last 5 Years of Life: A Retrospective Cohort Study of Decedents with Advanced Cancer and End-Stage Organ Diseases
Abstract
Background: Patients with nonmalignant end-stage organ diseases often incur healthcare costs in the last year of life that are disproportionately higher than in the period prior. Studies on healthcare expenditure (HCE) trends in these patients have largely focused on the final year of life, and examining a longer-term trajectory could better support healthcare professionals to target the timing and methods of care management. In this study, we aim to describe the HCE trajectories of end-stage organ disease (ESOD) over the last 5 years of life, compared against advanced cancer (AC).
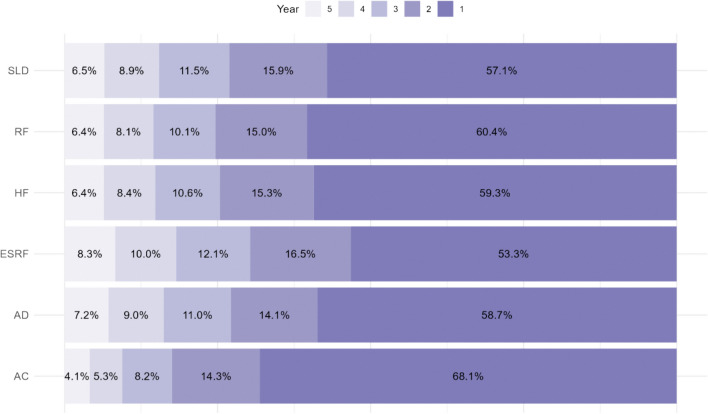
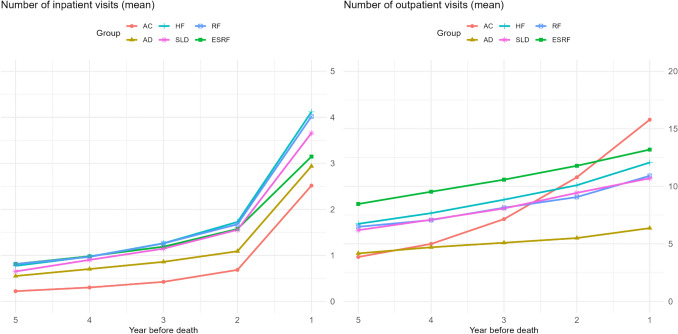
Methods: We conducted a retrospective cohort study to profile decedents who had either a primary or secondary diagnosis of AC, advanced dementia, severe liver disease, as well as heart failure (HF), end-stage renal failure (ESRF), or respiratory failure (RF) in the last 5 years of their lives using a regional health system database in Singapore. Hospital-based HCE and utilization for each diagnosis group was reported cumulatively for 5 years, by year and by month. The proportion of the 5-year HCE incurred in each year was also reported.
Results: Across all conditions, monthly HCE started to increase rapidly around 3 years prior to death, with 80% of the 5-year expenditure incurred in the same period. Expenditure among patients with ESODs other than dementia was £12,787 to £21,019 higher in comparison with patients with AC. Patients with RF incurred the highest 5-year HCE, driven by inpatient admissions.
Conclusions: Our findings highlight the importance of examining HCE trends in ESOD and their cost drivers over multiple years prior to the last year of life to inform healthcare policy and to review care processes to ensure appropriate and efficient end-of-life (EOL) care.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Funding: This work was supported by the Palliative Care Centre for Excellence in Research and Education [grant no. PalC-RG-22/P002]. The funder had no involvement in any aspect of this study or decision to publish. Conflicts of Interest: The authors declare that they have no conflicts of interest. Availability of Data and Materials: The datasets generated and/or analyzed during the current study are not publicly available owing to NHG’s data protection policies to ensure data privacy of patients. Statistical code used and aggregate data may be made available from the corresponding author on reasonable request. Ethics Approval and Consent to Participate: Exemption from review was granted by the review board of the National Healthcare Group (Domain Specific Review Board Study reference no. 2022/00663), as the research involved analysis of datasets without identifiers. A waiver for obtaining informed consent from patients was hence granted. Consent for Publication: Not applicable. Author Contributions: S.H.X.N., L.T.L.C., M.K.Y.H., A.H.Y.H., T.W.S., and A.H. contributed to the conceptualization of the study and funding acquisition. S.H.X.N. acquired and analyzed the data. S.N.H.X. drafted the article, with critical revision by P.K., T.R.Y., L.T.L.C., A.H.Y.H., T.W.S., and A.H. All authors read and approved the current version of the article to be published.
Figures

References
-
- Fassbender K, Fainsinger RL, Carson M, Finegan BA. Cost trajectories at the end of life: the Canadian experience. J Pain Symptom Manage. 2009;38(1):75–80. - PubMed
-
- Cohen-Mansfield J, Skornick-Bouchbinder M, Brill S. Trajectories of end of life: a systematic review. J Gerontol B Psychol Sci Soc Sci. 2018;73(4):564–72. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
