

Effect of a Telemedicine Model on Patients With Heart Failure With Reduced Ejection Fraction in a Resource-Limited Setting in Vietnam: Cohort Study
- PMID: 40106810
- PMCID: PMC11966076
- DOI: 10.2196/67228
Effect of a Telemedicine Model on Patients With Heart Failure With Reduced Ejection Fraction in a Resource-Limited Setting in Vietnam: Cohort Study
Abstract
Background: Heart failure (HF) is a complex, life-threatening condition marked by high morbidity, mortality, reduced functional capacity, poor quality of life, and substantial health care costs. HF with reduced ejection fraction (HFrEF) represents the subgroup of HF with the highest risks of mortality and hospitalization, necessitating the prioritization of care and management models to optimize treatment outcomes in these patients. Currently, data on the effectiveness of telemedicine models in resource-limited settings, such as low- and middle-income countries, are scarce.
Objective: This study aimed to evaluate the impact of telemedicine on improving prognosis in patients with HFrEF in Vietnam.
Methods: In this prospective cohort study, we recruited patients who received either remote monitoring and management (telemedicine) or standard monitoring and management (usual care) in the outpatient department of the Vietnam National Heart Institute, Bach Mai Hospital, Hanoi, Vietnam. Eligible patients were ≥18 years old, had a diagnosis of HFrEF defined as left ventricular ejection fraction (LVEF) ≤40%, had a history of HF hospitalization within the past 12 months, and presented with clinical symptoms classified as New York Heart Association (NYHA) II or III. The primary composite outcome was defined as the time to the first unplanned HF hospitalization or all-cause mortality. The follow-up period for all outcomes extended to 12 months.
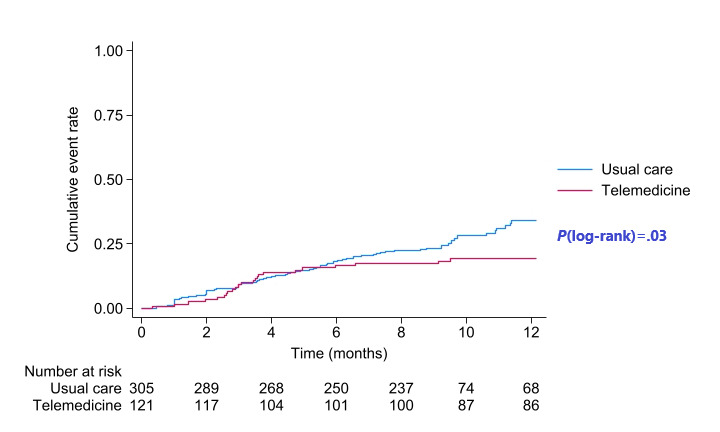
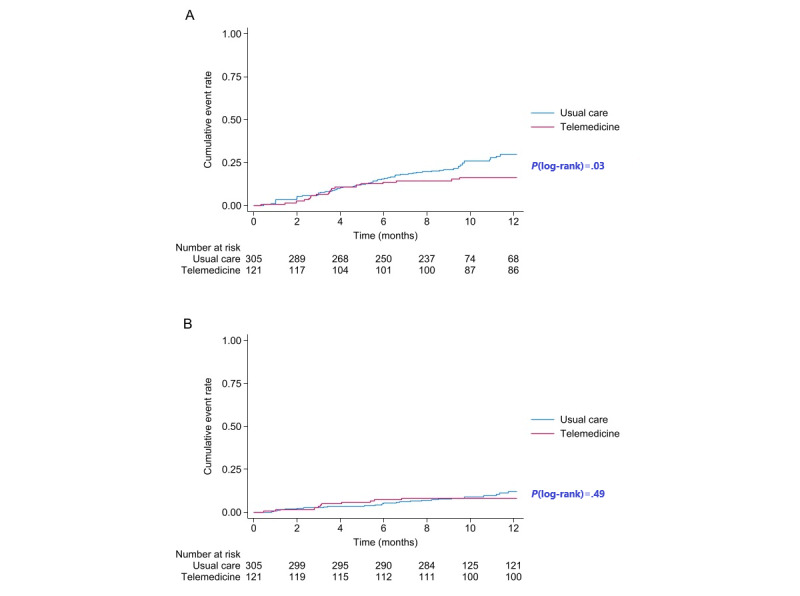
Results: In total, 426 patients (298/426, 70% male; 128/426, 30% female) with a mean age of 61.3 (SD 14.6) years and a mean LVEF of 32.1% (SD 6.0%) were included in our study. Of these patients, 121 received telemedicine care, while 305 received usual care. The primary outcome occurred in 23 (23/121, 19%) patients in the telemedicine group and 82 (82/305, 26.9%) patients in the usual care group during the follow-up period, indicating a significant reduction in risk (adjusted hazard ratio [aHR] 0.57, 95% CI 0.35-0.94; P=.03). However, this effect was primarily driven by a significant reduction in unplanned HF hospital admissions (aHR 0.57, 95% CI 0.33-0.98; P=.04) rather than in all-cause mortality (aHR 0.77, 95% CI 0.36-1.63; P=.49).
Conclusions: This study demonstrates that a simplified telemedicine model, even in resource-limited settings such as Vietnam, can effectively facilitate the remote monitoring and management of patients with HFrEF, resulting in significant reductions in HF-related hospitalizations and all-cause mortality.
Trial registration: National Agency for Science and Technology Information (NASATI), Vietnam CT07/01-2022-3; https://nsti.vista.gov.vn/projects/dth/xay-dung-mo-hinh-theo-doi-va-tu-van-suc-khoe-tim-mach-tu-xa-tai-thanh-pho-ha-noi-109276.html.
Keywords: HFrEF; Vietnam; all-cause mortality; cardiology; cardiovascular disease; cohort; cost-effective; heart; heart failure; heart failure hospitalization; hospitalization; low-cost; monitoring; mortality; remote; remote management; remote monitoring; resource-limited; telecare; telehealth; telemedicine.
©Hoai Thi Thu Nguyen, Hieu Ba Tran, Phuong Minh Tran, Hung Manh Pham, Co Xuan Dao, Thanh Ngoc Le, Loi Doan Do, Ha Quoc Nguyen, Thom Thi Vu, James Kirkpatrick, Christopher Reid, Dung Viet Nguyen. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 19.03.2025.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Efficacy of telemedical interventional management in patients with heart failure (TIM-HF2): a randomised, controlled, parallel-group, unmasked trial.Lancet. 2018 Sep 22;392(10152):1047-1057. doi: 10.1016/S0140-6736(18)31880-4. Epub 2018 Aug 25. Lancet. 2018. PMID: 30153985 Clinical Trial.
-
Impact of telemedical management on hospitalization and mortality in heart failure patients with diabetes: a post-hoc subgroup analysis of the TIM-HF2 trial.Cardiovasc Diabetol. 2024 Jun 12;23(1):198. doi: 10.1186/s12933-024-02285-0. Cardiovasc Diabetol. 2024. PMID: 38867198 Free PMC article. Clinical Trial.
-
Characteristics and Outcomes of Adult Outpatients With Heart Failure and Improved or Recovered Ejection Fraction.JAMA Cardiol. 2016 Aug 1;1(5):510-8. doi: 10.1001/jamacardio.2016.1325. JAMA Cardiol. 2016. PMID: 27434402
-
A facilitated home-based cardiac rehabilitation intervention for people with heart failure and their caregivers: a research programme including the REACH-HF RCT.Southampton (UK): NIHR Journals Library; 2021 Feb. Southampton (UK): NIHR Journals Library; 2021 Feb. PMID: 33617178 Free Books & Documents. Review.
-
Atrial fibrillation and risk of adverse outcomes in heart failure with reduced, mildly reduced, and preserved ejection fraction: A systematic review and meta-analysis.J Cardiovasc Electrophysiol. 2024 Apr;35(4):715-726. doi: 10.1111/jce.16209. Epub 2024 Feb 13. J Cardiovasc Electrophysiol. 2024. PMID: 38348517
Cited by
-
Application of AI Chatbot in Responding to Asynchronous Text-Based Messages From Patients With Cancer: Comparative Study.J Med Internet Res. 2025 May 21;27:e67462. doi: 10.2196/67462. J Med Internet Res. 2025. PMID: 40397947 Free PMC article.
References
-
- Bozkurt B, Coats AJ, Tsutsui H, Abdelhamid M, Adamopoulos S, Albert N, Anker SD, Atherton J, Böhm Michael, Butler J, Drazner MH, Felker GM, Filippatos G, Fonarow GC, Fiuzat M, Gomez-Mesa J, Heidenreich P, Imamura T, Januzzi J, Jankowska EA, Khazanie P, Kinugawa K, Lam CSP, Matsue Y, Metra M, Ohtani T, Francesco Piepoli M, Ponikowski P, Rosano GMC, Sakata Y, SeferoviĆ P, Starling RC, Teerlink JR, Vardeny O, Yamamoto K, Yancy C, Zhang J, Zieroth S. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J Card Fail. 2021 Mar 01;:1. doi: 10.1016/j.cardfail.2021.01.022.S1071-9164(21)00050-6 - DOI - PubMed
-
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm Michael, Burri H, Butler J, Čelutkienė J, Chioncel O, Cleland JGF, Coats AJS, Crespo-Leiro MG, Farmakis D, Gilard M, Heymans S, Hoes AW, Jaarsma T, Jankowska EA, Lainscak M, Lam CSP, Lyon AR, McMurray JJV, Mebazaa A, Mindham R, Muneretto C, Francesco Piepoli M, Price S, Rosano GMC, Ruschitzka F, Kathrine Skibelund A, ESC Scientific Document Group 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021 Sep 21;42(36):3599–3726. doi: 10.1093/eurheartj/ehab368. https://hdl.handle.net/2268/290864 6358045 - DOI - PubMed
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, Elkind MSV, Evenson KR, Ferguson JF, Gupta DK, Khan SS, Kissela BM, Knutson KL, Lee CD, Lewis TT, Liu J, Loop MS, Lutsey PL, Ma J, Mackey J, Martin SS, Matchar DB, Mussolino ME, Navaneethan SD, Perak AM, Roth GA, Samad Z, Satou GM, Schroeder EB, Shah SH, Shay CM, Stokes A, VanWagner LB, Wang N, Tsao CW, American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021 Feb 23;143(8):e254–e743. doi: 10.1161/CIR.0000000000000950. https://www.ahajournals.org/doi/abs/10.1161/CIR.0000000000000950?url_ver... - DOI - DOI - PubMed
-
- Shahim B, Kapelios CJ, Savarese G, Lund LH. Global public health burden of heart failure: an updated review. Card Fail Rev. 2023;9:e11. doi: 10.15420/cfr.2023.05. https://europepmc.org/abstract/MED/37547123 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
