

Costs and Complications of Respiratory Syncytial Virus and Acute Respiratory Infections in the Adult Population: Analysis of a German Claims Database
- PMID: 40108096
- PMCID: PMC12037943
- DOI: 10.1007/s41669-025-00565-3
Costs and Complications of Respiratory Syncytial Virus and Acute Respiratory Infections in the Adult Population: Analysis of a German Claims Database
Abstract
Background: Respiratory syncytial virus (RSV) infections pose health and economic burdens to adults. Using claims data, we estimated RSV-associated costs, healthcare resource utilization (HCRU), and complication rates from patients of a nationwide German health insurance database.
Methods: We analyzed confirmed RSV, RSV-possible, and acute respiratory infection (ARI) cohorts, plus 1:1 matched control cohorts of individuals ≥ 18 years from 2010 to 2019. Matching was performed separately for patients 18-49, 50-59, and ≥ 60 years. Medical costs, HCRU, and sick leave were assessed for inpatients and outpatients. Complications were compared between cases and controls, and logistic regression assessed odds ratios (ORs) for risk.
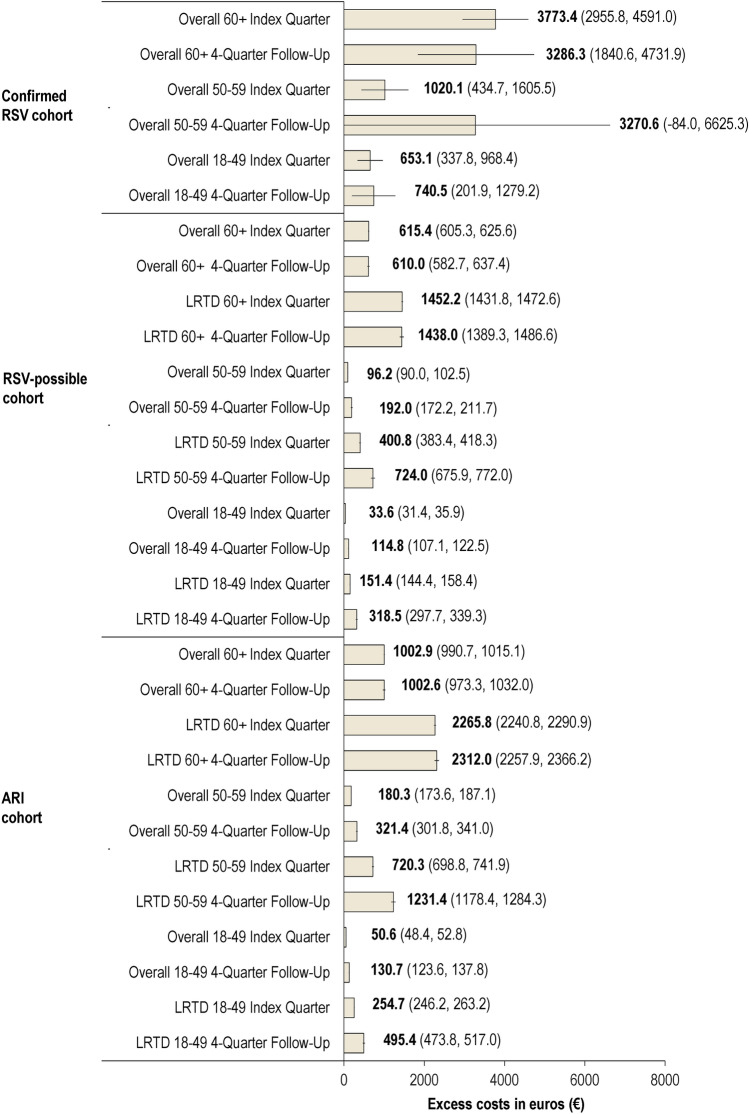
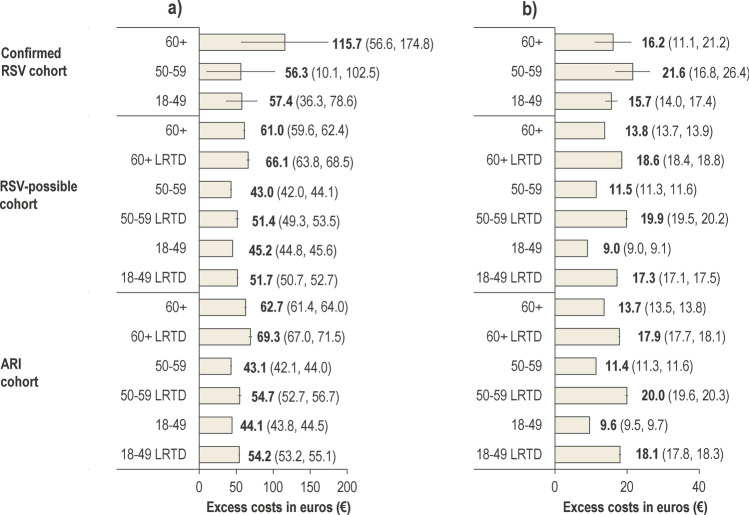
Results: Altogether, 2668 confirmed RSV index episodes occurred. In ≥ 60-year-olds, 862 episodes incurred mean excess costs of €3773 (95% confidence interval [CI]: €2956-€4591) per episode during the index quarter and €3286 (95% CI: €1841-€4732) in the following four quarters. Mean costs were €5553 per episode for inpatients and €116 for outpatients. In ≥ 60-year-olds, risk for congestive heart failure hospitalization (OR 2.3; 95% CI: 1.4-3.8), exacerbation of asthma (OR 6.0; 95% CI: 1.7-20.9), and chronic obstructive pulmonary disease (OR 3.9; 95% CI: 2.6-5.8) were higher for confirmed RSV than controls. In younger groups, costs, HCRU, and complications were also higher in cases than controls. The complication frequencies increased with age. RSV-possible episodes incurred mean excess costs of €615 (95% CI: €605-€626) during the index quarter and €610 (95% CI: €583-€637) during the following four quarters, while in the ARI cohort, the excess costs were €1003 (95% CI: €991-€1015) during the index quarter and €1003 (95% CI: €973-€1032) in the following four quarters. For all three cohorts, individuals who had comorbidities, were immunocompromised, or living in long-term care facilities incurred higher costs.
Conclusions: Confirmed RSV is associated with high excess costs - especially in hospital settings - and HCRU. Complication risk increased with RSV presence.
© 2025. GSK Plc.
Conflict of interest statement
Declarations. Funding: GSK funded this study (VEO-000566) and was involved in all stages of study conduct, including analysis of the data. GSK also took charge of all costs associated with the development and publication of this manuscript. Data availability: For requests for access to anonymized subject-level data, please contact the corresponding author. Competing Interests: MK, MW, SP, and PM are employed by GSK. AM, MJF, and MS are employed by GSK and hold financial equities in GSK. TL was employed by GSK at the time of the study and held financial equities in GSK, and is now employed by the National Health Care Institute, Diemen, Netherlands. AA received payment or honoraria for lectures from GSK. JS received consulting fees from GSK, MSD, Sanofi, Pfizer, Novavax, Bavarian Nordic, and Seqirus; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from GSK, MSD, Sanofi, Pfizer, BioNTech, Moderna, Novavax, Takeda, Bavarian Nordic, Viatris, Seqirus, Novartis, and Janssen; support for attending meetings and/or travel from Sanofi and Pfizer; participated on a Data Safety Monitoring Board or Advisory Board at GSK, MSD, Sanofi, Pfizer, Moderna, Novavax, Bavarian Nordic, and Viatris. SE received payment or honoraria for lectures and presentations from GSK; the author declares to be author and coauthor of respiratory guidelines (unpaid). CV received grants or contracts for his institution from the German Ministry of Education and Science (BMBF), AstraZeneca, Boehringer Ingelheim, Chiesi, CSL Behring, GSK, Grifols, and Novartis; consulting fees from Aerogen, AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, GSK, Insmed, Menarini, Novartis, Nuvaira, Roche, and Sanofi; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Aerogen, AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, GSK, Insmed, Menarini, Novartis, Roche, and Sanofi. NK is an employee of ZEG Berlin, which received funding from GSK for the conduct of the study. RK is an employee of WIG2, which received funding from GSK for the conduct of the study. RKo received grants or contracts for his institution from the German Ministry of Education and Science (BMBF), Bavarian government, Boehringer Ingelheim, Chiesi, CSL Behring, GSK, Grifols, and Bosch; consulting fees from AstraZeneca, Biontech, Boehringer Ingelheim, CSL Behring, Chiesi, GSK, Menarini, Nuvaira, Pfizer, and Sanofi; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, GSK, Menarini, Pfizer, PulmonX, and Sanofi. The authors declare no other financial and non-financial relationships and activities. Contributorship: All authors participated in the design or implementation or analysis; interpretation of the study; and the development of this manuscript. All authors had full access to the data and gave final approval before submission. All authors agree to be accountable for all aspects of the work. Trademarks: AREXVY is a trademark owned by or licensed to GSK. ABRYSVO is a trademark of Pfizer. mRESVIA is a trademark of Moderna. Previous congress activities: Poster presentation at Ethics and Economics in the Health Care System, the 16th annual conference of the German Health Economics Association (DGGÖ), 4-5 March 2024, Halle (Saale), Germany. Ethics Approval: Not applicable. Consent to Participate: Not applicable. Consent for Publication: Not applicable. Code Availability: Not applicable.
Figures
Similar articles
-
Economic burden of respiratory syncytial virus in adults in Germany - a health claims analysis between 2015 and 2018.J Med Econ. 2024 Jan-Dec;27(1):1063-1075. doi: 10.1080/13696998.2024.2389676. Epub 2024 Aug 19. J Med Econ. 2024. PMID: 39105626
-
Estimating the Economic Impact of Respiratory Syncytial Virus and Other Acute Respiratory Infections Among Infants Receiving Care at a Referral Hospital in Malawi.J Pediatric Infect Dis Soc. 2020 Dec 31;9(6):738-745. doi: 10.1093/jpids/piaa157. J Pediatric Infect Dis Soc. 2020. PMID: 33347578 Free PMC article.
-
Respiratory syncytial virus acute respiratory infections in ≥ 65-year-old adults in long-term care facilities in the Czech Republic.Cent Eur J Public Health. 2021 Sep;29(3):167-176. doi: 10.21101/cejph.a6861. Cent Eur J Public Health. 2021. PMID: 34623114
-
Global disease burden of and risk factors for acute lower respiratory infections caused by respiratory syncytial virus in preterm infants and young children in 2019: a systematic review and meta-analysis of aggregated and individual participant data.Lancet. 2024 Mar 30;403(10433):1241-1253. doi: 10.1016/S0140-6736(24)00138-7. Epub 2024 Feb 14. Lancet. 2024. PMID: 38367641
-
Cost of Respiratory Syncytial Virus-Associated Acute Lower Respiratory Infection Management in Young Children at the Regional and Global Level: A Systematic Review and Meta-Analysis.J Infect Dis. 2020 Oct 7;222(Suppl 7):S680-S687. doi: 10.1093/infdis/jiz683. J Infect Dis. 2020. PMID: 32227101
References
-
- RKI. RSV-Infektionen. 2024. Accessed: March 24, 2024. Available from: https://www.rki.de/DE/Content/Infekt/EpidBull/Merkblaetter/Ratgeber_RSV....
-
- Branche AR, Falsey AR. Respiratory syncytial virus infection in older adults: an under-recognized problem. Drugs Aging. 2015;32(4):261–9. 10.1007/s40266-015-0258-9. - PubMed
-
- Shi T, Denouel A, Tietjen AK, Campbell I, Moran E, Li X, et al. Global disease burden estimates of respiratory syncytial virus-associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis. 2020;222(Suppl 7):S577–83. 10.1093/infdis/jiz059. - PubMed
-
- Branche AR, Saiman L, Walsh EE, Falsey AR, Sieling WD, Greendyke W, et al. Incidence of respiratory syncytial virus infection among hospitalized adults, 2017–2020. Clin Infect Dis. 2022;74(6):1004–11. 10.1093/cid/ciab595. - PubMed
LinkOut - more resources
Full Text Sources
