

Impact of a training intervention on upper gastrointestinal endoscopy quality over time: Multicenter comparative cohort study
- PMID: 40109322
- PMCID: PMC11922177
- DOI: 10.1055/a-2526-0240
Impact of a training intervention on upper gastrointestinal endoscopy quality over time: Multicenter comparative cohort study
Abstract
Background and study aims: The European Society of Gastrointestinal Endoscopy (ESGE) and British Society of Gastroenterology (BSG) formulated performance measures to improve the detection rate for upper gastrointestinal (UGI) endoscopy. We aimed to assess adherence to and impact of training on adherence to performance measures for UGI endoscopy.
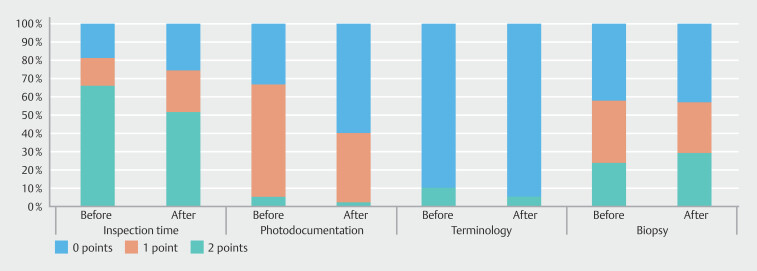
Methods: In this multicenter, prospective, cohort study, endoscopists at three centers underwent 1-hour face-to-face training based on ESGE and BSG procedure performance measures (≥ 7-minute inspection time; photodocumentation of ≥ 10 anatomical landmarks + abnormalities; standardized terminology; biopsy protocols). A self-developed quality assessment score was used to assess diagnostic UGI endoscopies before (control group) and after (intervention group) training. The primary endpoint was improvement in overall quality score (percentage of the maximum score).
Results: Of 1,733 consecutive UGI endoscopies, 570 were eligible for inclusion (mean patient age 60 years [standard deviation 15]; male 47%): 285 in the control group and 285 in the intervention group. Overall quality score increased from 60% before to 67% after the training intervention (difference 7%, 95% confidence interval [CI] 5-10, P < 0.001). Male patients (3.2%, 95% CI 0.7-5.7), alarming features (-3.1%, 95% CI -5.6 to -0.5), and endoscopist age (-0.4% increment per year, 95% CI -0.8 to -0.1) were associated with higher quality scores.
Conclusions: Adherence to the ESGE and BSG procedure performance measures for UGI endoscopy persistently increased after a 1-hour face-to-face training intervention, suggesting that a simple training intervention tool can improve the quality of UGI endoscopy and potentially could prevent missed lesions.
Keywords: Endoscopy Upper GI Tract; Image and data processing, documentatiton; Performance and complications; Quality and logistical aspects; Quality management; Training.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
Conflict of Interest PS has received research funding from Pentax, The E-Nose company, Lucid Diagnostics, Micro-Tech, Magentiq Eye, Norgine and Endo Tools Therapeutics, and consultancy fees from Magentiq Eye. LK, JvB, FI, RS and ML have no conflicts of interests.
Figures



References
-
- Nasseri-Moghaddam S, Mousavian A-H, Kasaeian A et al.What is the prevalence of clinically significant endoscopic findings in subjects with dyspepsia? Updated systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022;21:1739–1749. - PubMed
-
- Kaminski MF, Siwan T-G, Bugajski M et al.Performance measures for lower gastrointestinal endoscopy: a European Society of Gastrointestinal Endoscopy (ESGE) quality improvement initiative. Endoscopy. 2017;49:378–397. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous