

Multidimensional pain assessment and opioid use after total knee arthroplasty: continuous vs single-injection regional vs systemic analgesia
- PMID: 40109369
- PMCID: PMC11922405
- DOI: 10.1097/PR9.0000000000001257
Multidimensional pain assessment and opioid use after total knee arthroplasty: continuous vs single-injection regional vs systemic analgesia
Abstract
Introduction: Effective pain management after total knee arthroplasty (TKA) is essential for recovery. Continuous peripheral nerve blocks (PNBc) are often believed to provide superior pain relief compared with single-injection peripheral nerve blocks (PNBs). However, multidimensional pain-related patient-reported outcomes (PROs) have not been extensively studied.
Objective: Based on registry data, this study compared pain intensities summarized as a pain composite score (PCS) and postoperative opioid use between PNBc and PNBs nerve blocks in patients undergoing TKA, and evaluated additional PROs.
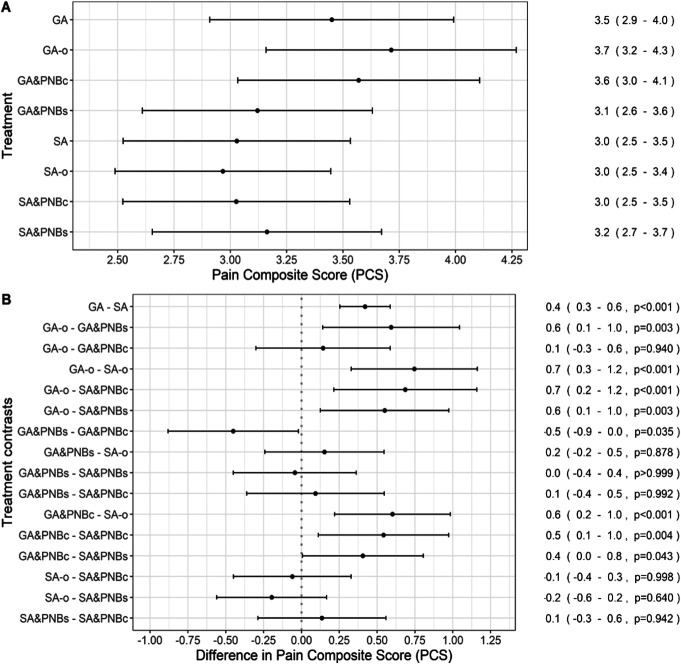
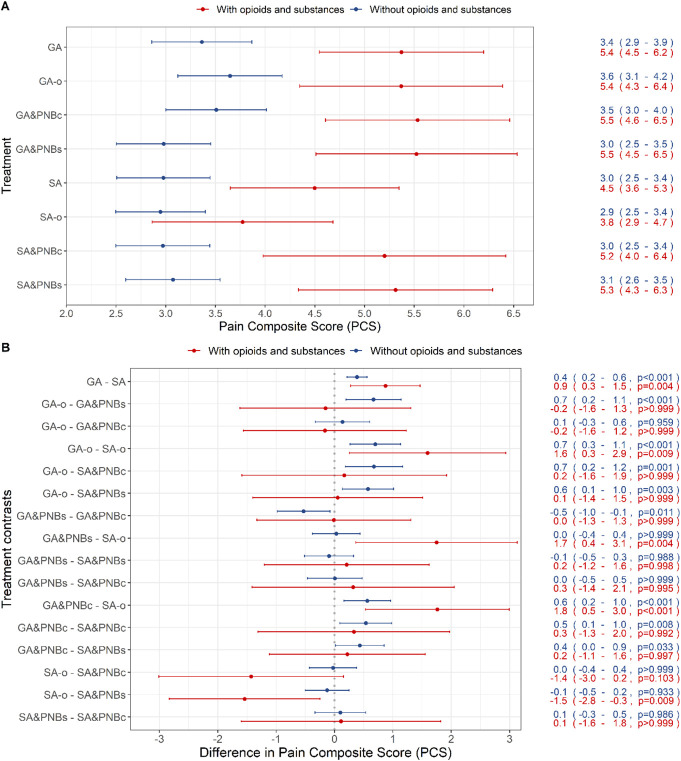
Methods: Data from 4,328 adults undergoing TKA enrolled in the PAIN OUT registry (ClinicalTrials.gov NCT02083835) were analyzed. Patients were categorized into general anesthesia (GA) or spinal anesthesia (SA), with subgroups general anesthesia only (GA-o) or spinal anesthesia only (SA-o), and combinations with single-injection PNB (GA&PNBs and SA&PNBs) or continuous PNB via catheter (GA&PNBc and SA&PNBc). The primary end point was PCS, summarizing pain intensities and time in severe pain during the first 24 hours. Secondary end points included opioid use and additional PROs.
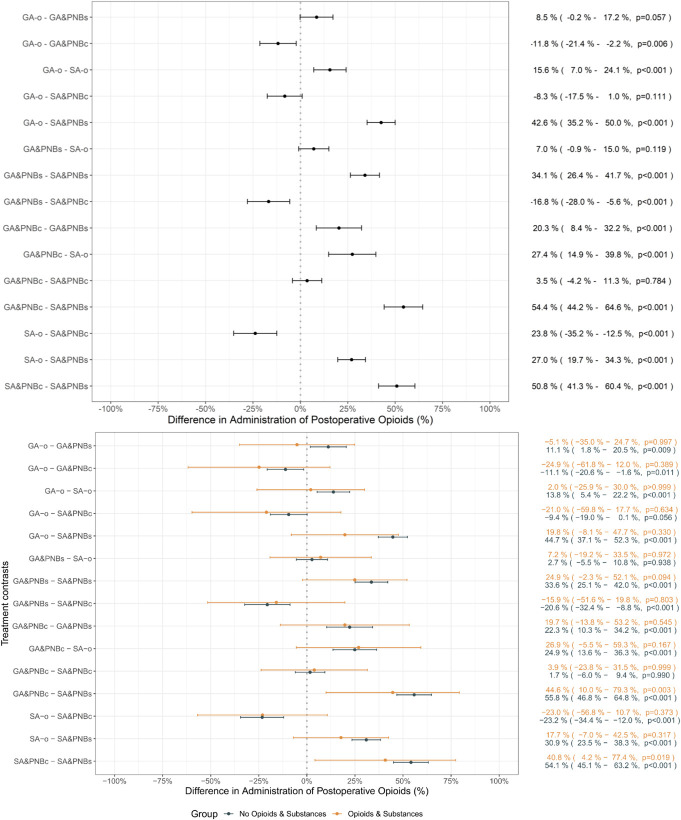
Results: The use of GA&PNBc was associated with a higher PCS (+0.5 [0.0-0.9], P = 0.035) compared with GA&PNBs, while PCS was similar between SA&PNBs and SA&PNBc. Opioid use was more frequent in GA&PNBc (+20.3%) and SA&PNBc (+50.8%) compared with the respective PNBs groups (P < 0.001). Patient-reported outcomes were higher in PNBc groups (median score 3.2 vs 2.7-2.9 in other groups; P < 0.001).
Conclusion: Continuous PNBc showed no clear advantage over PNBs in pain relief, opioid use, or further PROs. Future research should incorporate comprehensive PROs to better evaluate analgesic techniques in TKA.
Keywords: Assessment of pain/pain assessment; Continuous peripheral nerve block; Multidimensional pain scores; Opioid use; Pain-related patient-reported outcomes; Peripheral nerve block; Postoperative pain management; Total knee arthroplasty.
Copyright © 2025 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of The International Association for the Study of Pain.
Conflict of interest statement
U. M. Stamer serves as the Subforum Lead for Acute and Chronic Pain and Palliative Medicine (2020-2023) within the European Society of Anaesthesiology and Intensive Care (ESAIC) and as the Lead of the Acute Pain Working Group for the German Pain Society. The other authors have no conflict of interest to declare.
Figures
References
-
- Althaus A, Arránz Becker O, Neugebauer E. Distinguishing between pain intensity and pain resolution: using acute post-surgical pain trajectories to predict chronic post-surgical pain. Eur J Pain 2014;18:513–21. - PubMed
-
- Benzon HT, Mascha EJ, Wu CL. Studies on postoperative analgesic efficacy: focusing the statistical methods and broadening outcome measures and measurement tools. Anesth Analg 2017;125:726–8. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous