

Impact of DRG policy on the performance of tertiary hospital inpatient services in Chongqing, China: an interrupted time series study, 2020-2023
- PMID: 40109424
- PMCID: PMC11922081
- DOI: 10.3389/fpubh.2025.1523067
Impact of DRG policy on the performance of tertiary hospital inpatient services in Chongqing, China: an interrupted time series study, 2020-2023
Abstract
Background: Implementing the diagnosis-related groups (DRG) payment policy in 2021 marked a significant step in increasing the capacity and efficiency of public hospital services in Chongqing, China. However, the adaptability and effectiveness of DRG policy in middle-income regions like Chongqing remain understudied. This study evaluates the impact of DRG on tertiary hospital inpatient services in Chongqing, focusing on challenges unique to resource-constrained settings.
Methods: Using an interrupted time series design, we analyzed monthly data of 14 DRG performance measures obtained from the DRG comprehensive management system, covering two public hospitals in Chongqing from 2020 to 2023. To evaluate both immediate and long-term effects of the DRG policy, we employed an interrupted time series analysis model to analyze changes in indicator levels and trends pre- and post-intervention.
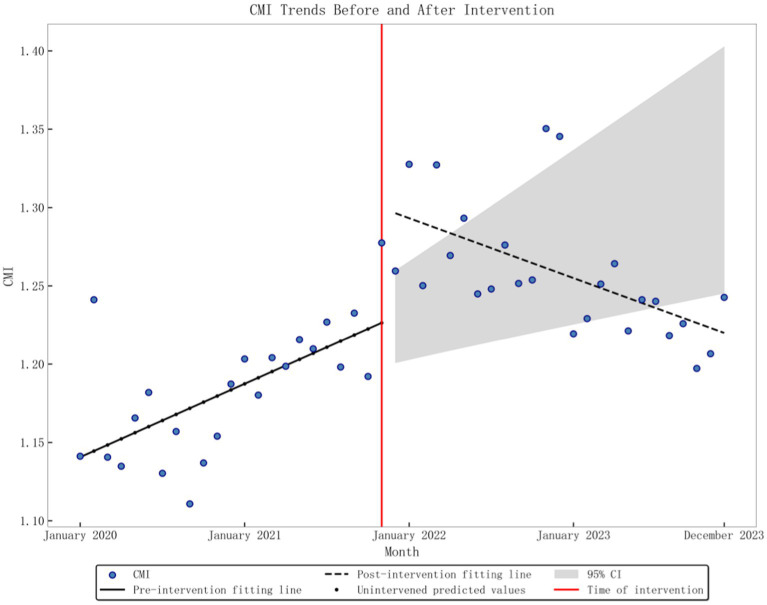
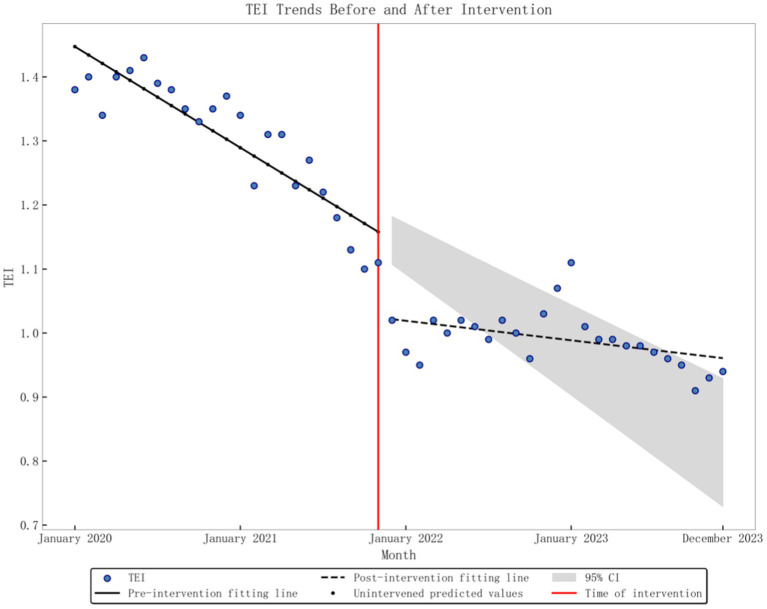
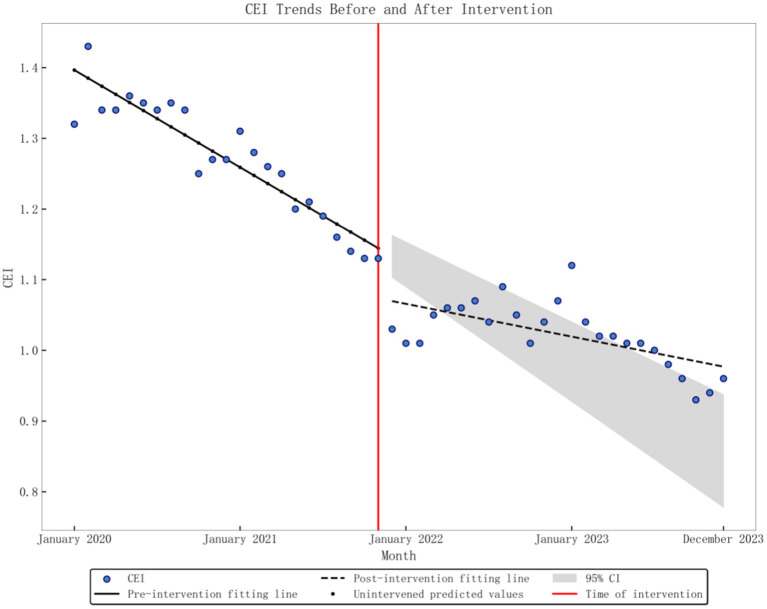
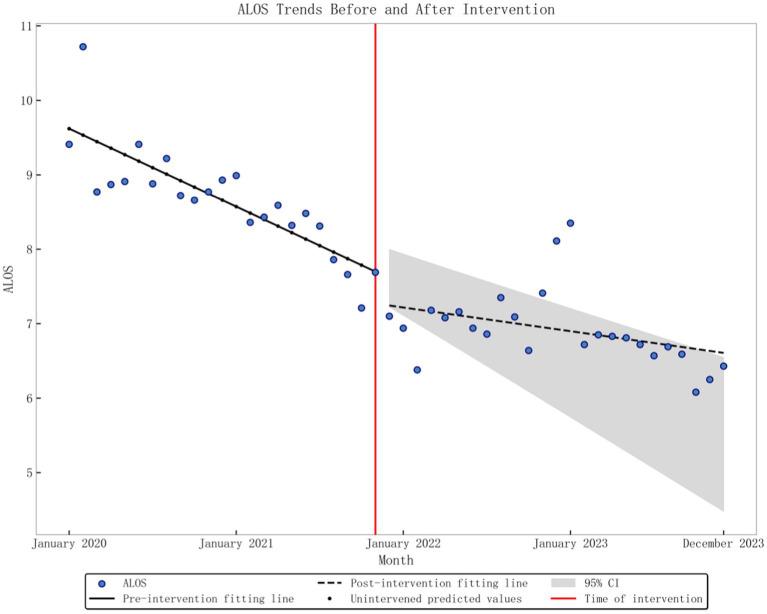
Results: We found significant changes in the following indicators since the implementation of the DRG policy: case-mix index (CMI) level increased by 0.0661 (p = 0.02), but the trend decreased by 0.0071 (p < 0.001). The time efficiency index (TEI) level decreased by 0.123 (p < 0.001), while the trend increased by 0.0106 (p < 0.001). The cost efficiency index (CEI) level decreased by 0.0633 (p = 0.003), with the trend rising by 0.0076 (p < 0.001). And average length of stay (ALOS) trend increased by 0.0609 (p = 0.002). Readmission rates (RR) exhibited an instantaneous increase of 0.5653% (p = 0.008) post-intervention, though the long-term trend remained stable (p = 0.598). No significant differences were observed in the changes in inpatient numbers, surgical proportion, bed turnover rate (BTR), mortality rates (DR), cost per hospitalization (CPH), drug cost per hospitalization (DCPH), consumable cost per hospitalization (CCPH), medical examination cost per hospitalization (MECPH), or medical service cost per hospitalization (MSCPH).
Conclusion: The DRG policy in Chongqing led to unintended trade-offs: tertiary hospitals prioritized high-volume, low-complexity cases, eroding service capacity for severe conditions. Middle-income regions faced implementation barriers, including fragmented health IT systems and insufficient administrative capacity, which diminished policy effectiveness. Policymakers must tailor DRG implementation to local contexts, balancing efficiency with equity and quality.
Keywords: DRG; performance evaluation; service capacity; service cost interrupted time series; service efficiency.
Copyright © 2025 Liu, Liao, Tan, Yan and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials