

Visual simulation of intraocular lenses: technologies and applications [Invited]
- PMID: 40109531
- PMCID: PMC11919339
- DOI: 10.1364/BOE.546971
Visual simulation of intraocular lenses: technologies and applications [Invited]
Abstract
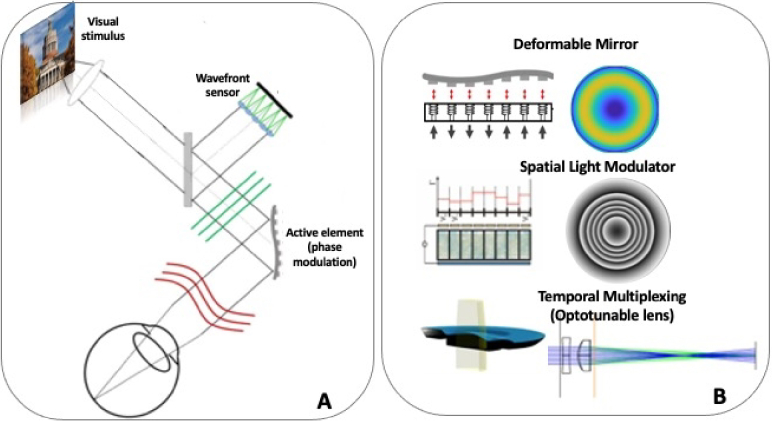
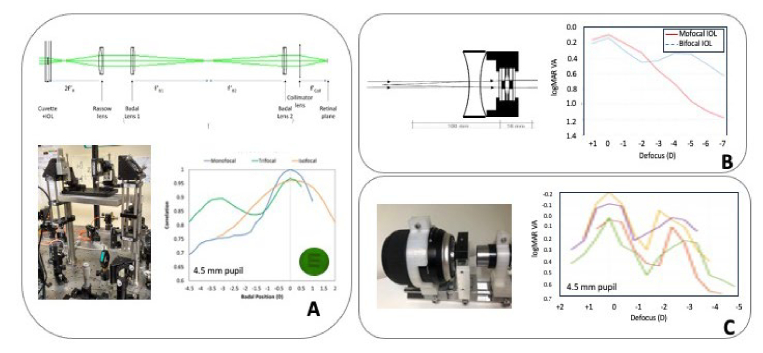
Cataract surgery requires selecting an intraocular lens (IOL), whose design affects visual outcomes. Traditional IOL evaluation relies on optical models and bench testing, but these methods fall short in simulating perceptual factors crucial to patient experience. Visual simulators, based on different principles including adaptive optics, temporal multiplexing or physical projection of the IOLs, now allow patients and clinicians to preview and compare different IOL designs preoperatively. By simulating real-world interactions of the eye's optics and the visual system with IOLs, these simulators enhance the patient decision-making process, enable personalized cataract surgery, and can aid in regulatory assessments of IOLs by incorporating pre-operative patient-reported visual outcomes. Visual simulators incorporate deformable mirrors, spatial light modulators and optotunable lenses as dynamic elements to simulate monofocal, multifocal and extended depth-of-focus IOLs, including newer designs aimed at improving contrast sensitivity, expanding depth of focus, and minimizing visual disturbances. With ongoing advancements, these simulators hold potential for transforming IOL design, regulatory processes, and patient care by providing realistic and patient-centered visual assessments, ultimately leading to more successful, individualized surgical outcomes.
© 2025 The Author(s).
Conflict of interest statement
SM discloses laboratory funding in areas related to IOLs and simulations from Alcon Research Labs (IO), BVI-PhysIOL (IO), Bausch and Lomb (UR), ClerioVision (UR); Coopervision (UR), Essilor International (IO), Johnson and Johnson (IO), Staar Surgical (IO), Meta Reality Labs (UR), Hoya (IO) for research with the described instruments. SM is a co-founder, shareholder and board member of 2EyesVision SL, a spin-off company of CSIC, which licenses related Vision Simulator technologies and is a co-inventor of patents P201730854, US9693679 and US10213358 licensed to 2EyesVision; SM is co-inventor of patent US10226327 and P201930791 (BVI/PhysIOL) and US2018042474 (Essilor) that used the described AO technology in their development. PA is a co-founder of Voptica SL, a start-up of the University of Murcia and co-inventor of patents US20120154742 and US20120038884 licensed to Voptica. LL discloses support from Johnson and Johnson; GY discloses support from Johnson and Johnson, Alcon..
Figures





References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources