

doi: 10.1055/a-2525-6768.
eCollection 2025.
Assessment of the Haemostatic Potential of Platelets Readied for Transfusion
Affiliations
- PMID: 40109577
- PMCID: PMC11922168
- DOI: 10.1055/a-2525-6768
Item in Clipboard
Assessment of the Haemostatic Potential of Platelets Readied for Transfusion
TH Open.
.
No abstract available
Conflict of interest statement
Conflict of Interest None declared.
Figures

Residual platelets in transfusion bags (<8 days old) were tested for response to agonists (maximum aggregation rate; MAR) using the Sinnowa PL-12 platelet function analyser. The agonists used were thrombin receptor-activating peptide (TRAP 32 μM,
n
= 16), arachidonic acid (AA; 0.2 mg/mL,
n
= 38), ADP (5 μM,
n
= 38; 50 μM,
n
= 16), and adrenaline (ADR; 100 μM,
n
= 14).
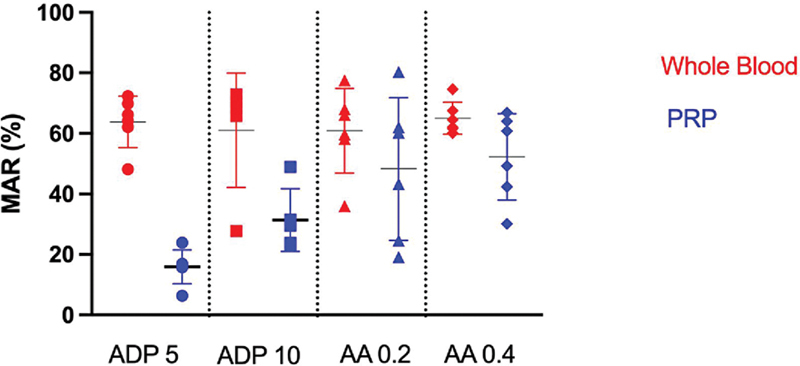
Blood was collected from healthy volunteers and PRP was prepared from it (
n
= 6). Both the blood and corresponding PRP were stimulated with ADP (5 and 10 μM) and arachidonic acid (0.2 and 0.4 mg/mL). The response to agonist is presented as maximum aggregation rate (MAR).
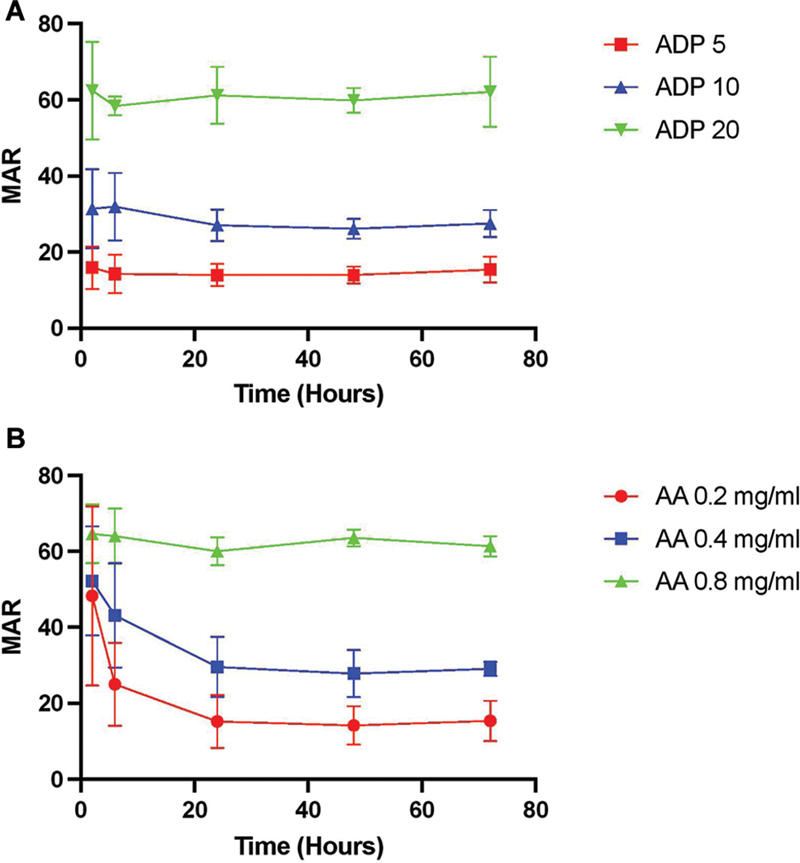
Blood was collected from healthy volunteers and PRP was prepared (
n
= 6) and stored at room temperature for 72 hours. PRP was stimulated with agonist immediately after preparing PRP (
t
= 0) and over 72 hours. Aggregation response is presented as maximum aggregation rate (MAR). (
A
) PRP stimulated with 5, 10, and 20 μM ADP. (
B
) PRP stimulated with 0.2. 0.4, and 0.8 mg/mL arachidonic acid.
References
-
- Banerjee S, Angiolillo D J, Boden W E et al.Use of antiplatelet therapy/DAPT for post-PCI patients undergoing noncardiac surgery. J Am Coll Cardiol. 2017;69(14):1861–1870. - PubMed
-
- Taylor G, Osinski D, Thevenin A, Devys J-M. Is platelet transfusion efficient to restore platelet reactivity in patients who are responders to aspirin and/or clopidogrel before emergency surgery? J Trauma Acute Care Surg. 2013;74(05):1367–1369. - PubMed
-
- Nagalla S, Sarode R. Role of platelet transfusion in the reversal of anti-platelet therapy. Transfus Med Rev. 2019;33(02):92–97. - PubMed
LinkOut - more resources
Full Text Sources