

Acute Myocardial Infarction and Stage E Shock: Insights From the RECOVER III Study
- PMID: 40109709
- PMCID: PMC11916721
- DOI: 10.1016/j.jscai.2024.102462
Acute Myocardial Infarction and Stage E Shock: Insights From the RECOVER III Study
Abstract
Background: The present analysis reports characteristics and outcomes of Society of Cardiovascular Angiography & Interventions (SCAI) stage E shock patients with acute myocardial infarction with cardiogenic shock (AMICS) undergoing percutaneous coronary intervention (PCI) who improved to stage C or D within 24 hours of Impella support ("responders") vs those patients who remained in stage E ("nonresponders").
Methods: The SCAI shock stage was assigned prior to initiation of Impella, and a second SCAI shock classification was performed within 24 hours of Impella support. SCAI shock stage was assigned independently by 2 reviewers; in cases where there was a discrepancy, a third reviewer adjudicated the stage assignment. Criteria such as a low pH (≤7.1), the need for multiple vasopressors/mechanical circulatory support devices, or the need for cardiopulmonary resuscitation were used to define stage E shock.
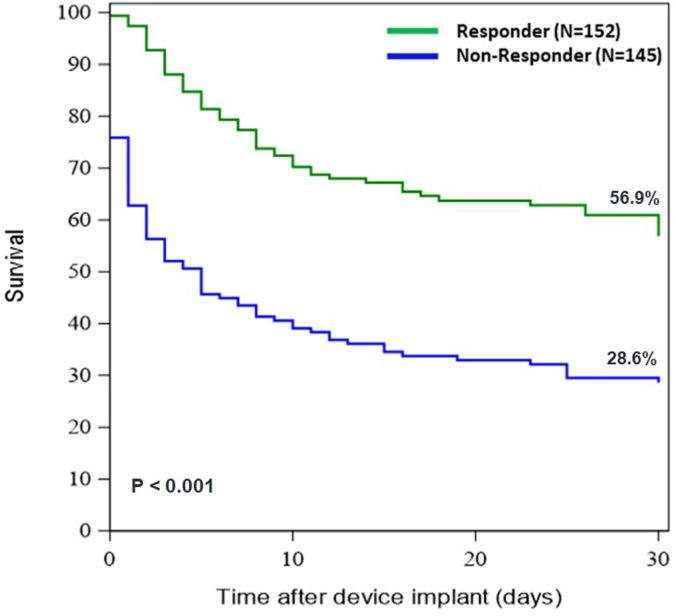
Results: Of the 415 RECOVER III patients, 298 presented in stage E shock; 152 (51.1%) were responders and 145 (48.8%) were nonresponders. Kaplan-Meier 30-day survival estimates were 56.9% and 28.6% in responders and nonresponders, respectively (P < .001). In multivariate analysis, fewer inotropic medications during Impella support (P < .0001), more lesions treated (P = .01), Impella support initiated pre-PCI (P = .03), and baseline white blood cell (P = .048) were all significant predictors for responsiveness to therapy.
Conclusions: Stage E patients who improved to stage C/D within 24 hours of Impella support had significantly better survival than those who remained in stage E. Predictors of responsiveness to therapy were mostly related to shock treatment strategy, and not baseline characteristics. This suggests that whether stage E patients will improve with Impella support is difficult to determine at the time support is initiated, and the SCAI shock stage should be repeated within 24 hours to more accurately determine the prognosis.
Keywords: SCAI shock class; acute myocardial infarction with cardiogenic shock; mechanical circulatory support; percutaneous coronary intervention.
© 2024 The Author(s).
Figures

References
-
- Hochman J.S., Sleeper L.A., Webb J.G., et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should we emergently revascularize occluded coronaries for cardiogenic shock. N Engl J Med. 1999;341(9):625–634. doi: 10.1056/NEJM199908263410901. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
