

Hearing Loss and Falls: A Systematic Review and Meta-Analysis
- PMID: 40111358
- PMCID: PMC11926736
- DOI: 10.1001/jamaoto.2025.0056
Hearing Loss and Falls: A Systematic Review and Meta-Analysis
Abstract
Importance: Falls constitute a significant public health concern worldwide and have been associated with increased morbidity and mortality across all ages. Identifying potentially modifiable risk factors for falls is a key public health priority. Literature surrounding the association between hearing loss (HL) and falls remains inconclusive.
Objective: To conduct a systematic review and meta-analysis to comprehensively synthesize evidence surrounding the impact of HL on falls.
Data sources: PubMed, Embase, and Cochrane Library from database inception through April 9, 2024.
Study selection: Observational studies investigating the association between HL and falls were selected. Only studies reporting covariate-adjusted estimates were included to minimize confounding.
Data extraction and synthesis: Two independent reviewers evaluated studies for eligibility, extracted data, and assessed the risk of bias of included studies. Using a random-effects model, adjusted estimates were pooled in meta-analyses. Heterogeneity was evaluated using subgroup and sensitivity analyses, and publication bias was assessed.
Main outcomes and measures: The cross-sectional odds and longitudinal risk of falls among patients with HL compared with those without HL.
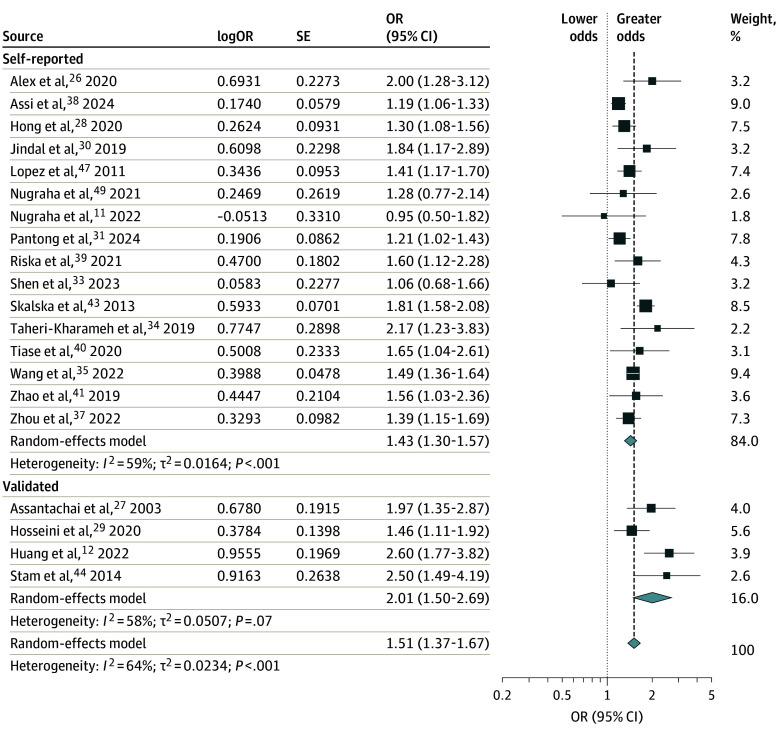
Results: A total of 5 071 935 participants were included from 27 studies; approximately 49.2% of participants were female, and 14 studies were conducted in Asia, 7 in North America, 3 in Europe, and 3 in Oceania, represented by Australia. Patients with HL exhibited an increased cross-sectional odds of falls (odds ratio, 1.51; 95% CI, 1.37-1.67; I2 = 64%) and longitudinal risk of falls (risk ratio, 1.17; 95% CI, 1.06-1.29; I2 = 69%) than those without HL. Further stratification by self-reported or validated hearing assessments, fall reporting duration, continent, community-dwelling adults, and studies adjusting for other sensory deficits identified as fall risk factors by the World Falls Guideline did not change significance. These results remained robust to sensitivity analyses, and publication bias was absent.
Conclusions and relevance: This systematic review and meta-analysis found that overall, HL may be a risk factor for falls. With a rapidly aging global population, it is crucial to acknowledge the public health concerns surrounding falls and consider if HL could be a potentially modifiable risk factor. Nonetheless, further randomized clinical trials are needed to elucidate any benefit of treating HL on fall prevention.
Conflict of interest statement
Figures



References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-1858. doi: 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- World Health Organization . Step safely: strategies for preventing and managing falls across the life-course. Accessed September 15, 2024. https://iris.who.int/bitstream/handle/10665/340962/9789240021914-eng.pdf
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
