

Sex-based differences in biomechanical function for chronic low back pain and how it relates to pain experience
- PMID: 40111489
- PMCID: PMC12213978
- DOI: 10.1007/s00586-025-08730-2
Sex-based differences in biomechanical function for chronic low back pain and how it relates to pain experience
Abstract
Purpose: The relationship between pain experience and biomechanical impairment in chronic low back pain (LBP) is unclear. Among the broader pain literature, sex-based differences in pain experience have been established. However, it is unknown if sex-based differences in pain experience relates to compromised movement patterns for patients with chronic LBP. This study examined sex differences and whether there are sex-based associations between pain experience and biomechanical function in patients with chronic LBP.
Methods: To capture the biomechanical variability among LBP patients, we quantified full-body movement quality based on the extent that 3D postural trajectories deviated from matched controls during a sit-to-stand task (Kinematic Composite Score, K-Score). For both males and females, the K-Score was compared to pain measures, including patient-reported metrics and quantitative sensory testing (pressure pain threshold, PPT).
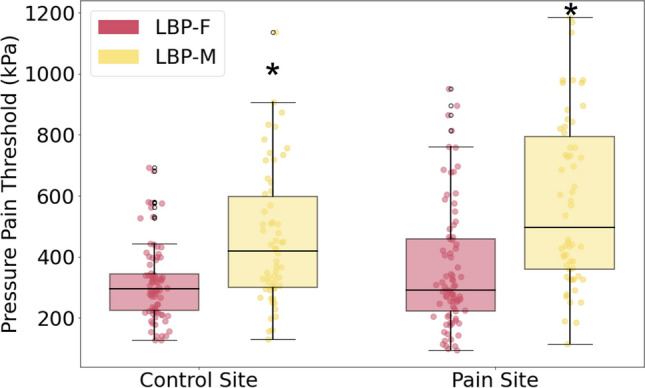
Results: There were significant sex-based differences in pain experience and biomechanical function in patients with LBP. Specifically, males exhibited ~ 8% lower trunk K-Scores, indicating biomechanical function that deviated more from controls when compared to female participants (p < 0.001). However, females exhibited PPT values 29% and 41% lower than males at the control and pain sites, respectively (p < 0.0001). There was a weak but significant negative association between PPT and K-Scores for males (R2 = 0.14, p < 0.01), while females lacked an association.
Conclusion: Overall, males with LBP exhibited worse movement quality, driven by trunk motion, but higher PPTs. Possible explanations include reduced interoceptive awareness or increased kinesiophobia in males, which may influence movement patterns. This research is an initial step in uncovering the complex relationship between patient-specific factors influencing LBP disability, laying the groundwork for further exploration, and paving the way for improving outcomes with patient-specific treatments.
Keywords: Biomechanics; Chronic low back pain; Composite score; Kinematics; Motion analysis; Motion capture; Pain experience; Quantitative sensory testing.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: RPM receives royalties from the University of California Regents for technology disclosures related to depth cameras. JFB has stock options with Bioniks, Limited Liability Company. GDO has received compensation as a member of the scientific advisory board of AT Dev Inc. and owns stock in the company. All other authors do not have any competing interest to declare.
Figures





References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
