

Parallel transmit 7T MRI for adult epilepsy pre-surgical evaluation
- PMID: 40112877
- PMCID: PMC12291008
- DOI: 10.1111/epi.18353
Parallel transmit 7T MRI for adult epilepsy pre-surgical evaluation
Abstract
Objective: To implement parallel transmit (pTx) 7T magnetic resonance imaging (MRI) in the pre-surgical evaluation of 3T-negative patients with drug-resistant focal epilepsy, and to compare quality to conventional single transmit (specifically, circularly polarized [CP]) 7T MRI.
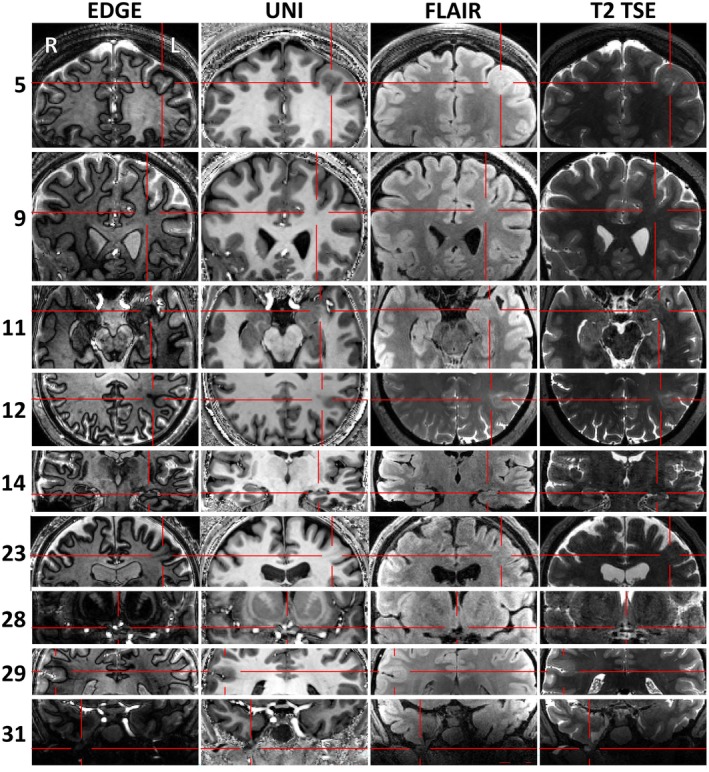
Methods: We implemented a comparative protocol comprising both pTx and CP 7T MRI in consecutive adult candidates for epilepsy surgery who had negative or equivocal 3T MRI imaging. Here we report the outcomes from the first 31 patients. We acquired pTx and CP T1, T2, fluid-attenuated inversion recovery (FLAIR) and edge-enhancing gradient echo (EDGE) images, all in the same three-dimensional (3D) 0.8 mm isotropic space. Two-dimensional (2D) high-resolution T2 and T2*-weighted sequences were acquired only in CP mode due to current technological limitations. Two neuroradiologists, a neurologist, and a neurosurgeon made independent, blinded quality and preference ratings of pTx vs CP images. Quantitative methods were used to assess signal dropout.
Results: 7T revealed previously-unseen structural lesions in nine patients (29%), confirmed 3T-equivocal lesions in four patients (13%), and disproved 3T-equivocal lesions in four patients (13%). Lesions were better visualized on pTx than CP in 57% of cases, and never better visualized on CP. Clinical management was altered by 7T in 18 cases (58%). Nine cases were offered surgical resection and one laser interstitial thermal therapy (LITT). Three cases were removed from the surgical pathway because of bilateral or extensive lesions. Five cases were offered stereo-electroencephalography (sEEG) with better targeting (in three because the 7T lesion was deemed equivocal by the multi-disciplinary team (MDT), and in two because the lesion was extensive). Blinded comparison confirmed significantly better overall quality of pTx FLAIR images (F(2, 184) = 13.7, p = 2.88 × 10-6), whereas pTx MP2RAGE images were subjectively non-inferior and had improved temporal lobe coverage with quantitatively less signal drop-out.
Significance: pTx-7T is implementable in a clinical pathway, changed management in 58% of patients where 3T + FDG-PET had not enabled resection, and is superior to single transmit 7T MRI.
Keywords: 7T MRI; epilepsy surgery; focal epilepsy; parallel transmit.
© 2025 The Author(s). Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
C.T.R. discloses research grant support from Siemens, for a different project. A.M. is employed by Siemens Healthcare SAS, Saint‐Denis, France. The remaining authors have no conflicts of interest. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Figures




References
-
- Ryvlin P, Cross JH, Rheims S. Epilepsy surgery in children and adults. Lancet Neurol. 2014;13:1114–1126. - PubMed
-
- Trattnig S, Bogner W, Gruber S, Szomolanyi P, Juras V, Robinson S, et al. Clinical applications at ultrahigh field (7T). Where does it make the difference? NMR Biomed. 2016;29:1316–1334. - PubMed
-
- van der Zwaag W, Schafer A, Marques JP, Turner R, Trampel R. Recent applications of UHF‐MRI in the study of human brain function and structure: a review. NMR Biomed. 2016;29:1274–1288. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
