

Indocyanine green fluorescence navigation with 4K overlay vs. conventional laparoscopic liver resection: a propensity score-matched analysis (liver-light study)
- PMID: 40113618
- PMCID: PMC12041050
- DOI: 10.1007/s00464-025-11671-y
Indocyanine green fluorescence navigation with 4K overlay vs. conventional laparoscopic liver resection: a propensity score-matched analysis (liver-light study)
Abstract
Introduction: Laparoscopic liver resection (LLR) has revolutionized liver surgery by offering several advantages over traditional open procedures. However, conventional LLR (C-LLR) has certain limitations, such as the inability to palpate tumors and the need for continuous ultrasound guidance during surgery, which can result in complications. Real-time tumor-tracking technologies, such as indocyanine green (ICG) fluorescence imaging, have shown potential in enhancing tumor detection and improving perioperative outcomes. The Liver-Light study aims to evaluate the feasibility of integrating ICG fluorescence with 4 K imaging technology during LLR (ICG4K-LLR) to improve postoperative surgical and oncological outcomes.
Methods: This study is a prospective, single-center investigation that included 42 patients who underwent ICG4K-LLR. These patients were matched in a 1:1 ratio using propensity scores with patients from retrospective data who underwent C-LLR. Potential confounding factors, including sex, age, body mass index, tumor type, and the complexity of LLR, were selected for matching. Postoperative surgical and oncological outcomes were then compared between the two groups.
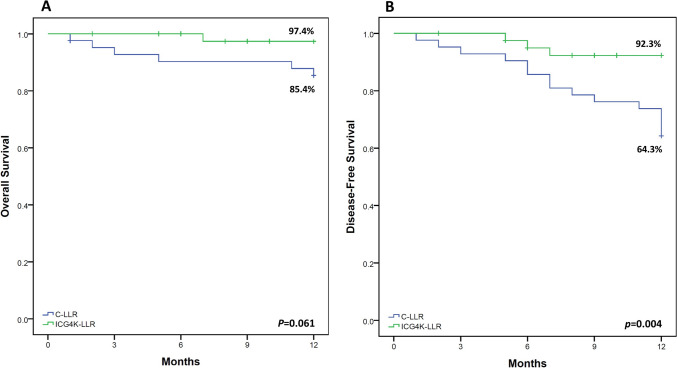
Results: After propensity score-matched analysis, the ICG4K-LLR group demonstrated several significant advantages over the C-LLR group. Operation times were shorter in the ICG4K-LLR group (155.2 min vs. 196.6 min, p = 0.002), with reduced blood loss (300.0 ml vs. 501.2 ml, p = 0.006) and fewer blood transfusions (0% vs. 14.3%, p = 0.011). Additionally, no patients in the ICG4K-LLR group had positive resection margins, whereas 14.3% of patients in the C-LLR group did (p = 0.011). The incidence of clinically relevant posthepatectomy liver failure (p = 0.040) and major morbidity (p = 0.035) was significantly lower in the ICG4K-LLR group. Furthermore, the 1-year disease free survival rate was significantly higher in the ICG4K-LLR group (92.3% vs. 64.3%, p = 0.004).
Conclusion: ICG4K-LLR has a promising potential as a safe and effective navigation system, offering improved perioperative surgical and oncological outcomes compared to C-LLR.
Keywords: 4 K technology; Hepatectomy; Indocyanine green; Laparoscopy; Navigation system.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Disclosures: Omid Ghamarnejad, Ghassan Batikha, Elias Khajeh, Hamraz Javaheri, Mahmoud Jabal, Rizky Widyaningsih, and Gregor Alexander Stavrou have no conflicts of interest or financial ties to disclose.
Figures



References
-
- Haney CM, Studier-Fischer A, Probst P, Fan C, Müller PC, Golriz M, Diener MK, Hackert T, Müller-Stich BP, Mehrabi A, Nickel F (2021) A systematic review and meta-analysis of randomized controlled trials comparing laparoscopic and open liver resection. HPB 23:1467–1481. 10.1016/j.hpb.2021.03.006 - DOI - PubMed
-
- Liu F, Wang H, Ma W, Li J, Liu Y, Tang S, Li K, Jiang P, Yang Z, He Y (2023) Short-and long-term outcomes of indocyanine green fluorescence navigation-versus conventional-laparoscopic hepatectomy for hepatocellular carcinoma: a propensity score-matched, retrospective, cohort study. Ann Surg Oncol 30:1991–2002 - DOI - PMC - PubMed
-
- Stavrou GA, Stang A, Raptis DA, Schadde E, Zeile M, Brüning R, Wagner KC, Huber TM, Oldhafer KJ (2021) Intraoperative (contrast-enhanced) ultrasound has the highest diagnostic accuracy of any imaging modality in resection of colorectal liver metastases. J Gastrointest Surg 25:3160–3169 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
