

Diagnostic accuracy in NSCLC lymph node staging with Total-Body and conventional PET/CT
- PMID: 40113643
- PMCID: PMC12222388
- DOI: 10.1007/s00259-025-07177-3
Diagnostic accuracy in NSCLC lymph node staging with Total-Body and conventional PET/CT
Abstract
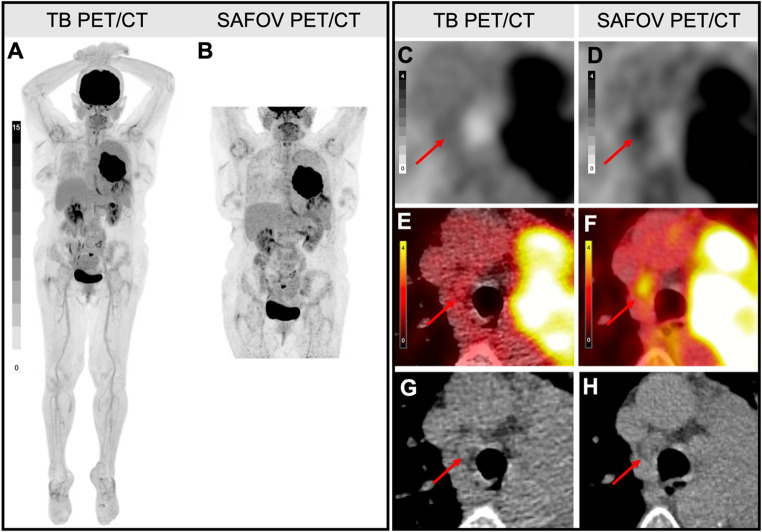
Introduction: Our aim was to characterize the diagnostic accuracy indices for nodal (N)-staging with [18F]FDG Total-Body (TB) and short-axial field-of-view (SAFOV) PET/CT in non-small cell lung cancer (NSCLC) patients referred for staging or restaging.
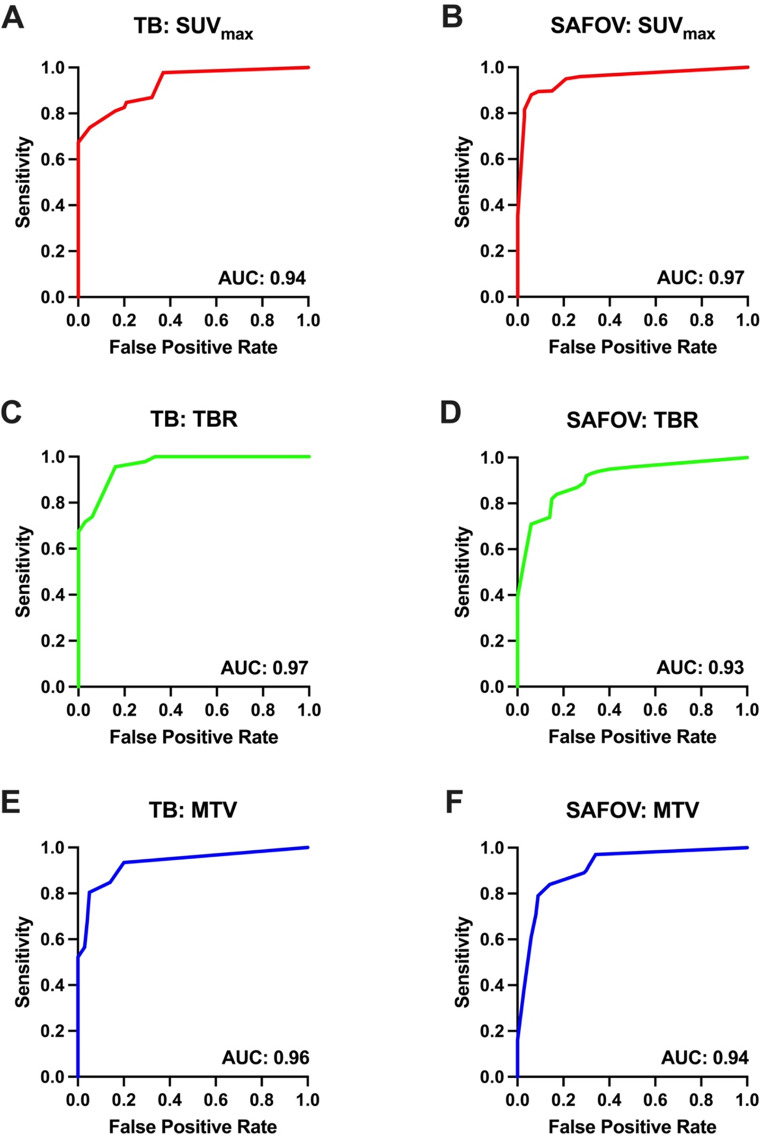
Methods: In this prospective single center cross-over head-to-head comparative study 48 patients underwent [18F]FDG TB and SAFOV PET/CT on the same day. In total 700 lymph node levels (1R/L, 2R/L, 3a/p, 4R/L, 5, 6, 7, 8R/L, 9R/L, 10-14R/L) of 28 patients could be correlated to a composite reference standard (histopathological correlation, imaging after localized or systemic treatment), which allowed determination of true positive (TP), false positive (FP), true negative (TN) and false negative (FN) lesions. Lymph nodes were characterized semi-quantitatively by maximum standardized uptake value (SUVmax), tumor-to-background ratio (TBR), metabolic tumor volume (MTV) and total lesion glycolysis (TLG) leading to threshold for each scanner.
Results: TB and SAFOV PET/CT showed high diagnostic accuracy indices for patient-based N-staging. Sensitivity and specificity were 86.0% (CI: 77.0-95.0%) and 98.3% (CI: 97.3-99.3%) for TB; 77.2% (CI: 66.3-88.1%) and 97.4% (CI: 96.1-98.6%) for SAFOV PET. Positive predictive value was higher for TB (81.7%, CI: 71.9-91.5%) compared to SAFOV PET (72.1%, CI: 60.9-83.4%). However, this finding was not statistically significant (p = 0.08). Negative predictive values for TB (98.6%, CI: 97.9-99.6%) and SAFOV PET/CT (98.0%, CI: 96.9-99.1%) were comparable. Overall, NSCLC N-staging was affected in six cases on SAFOV and only in one case on TB PET/CT. Semi-quantitative analysis revealed a threshold of SUVmax 3.0 to detect TP lesions on both scanners. However, TBR, MTV and TLG thresholds were lower on TB compared to SAFOV PET (TBR: 1.2 vs. 1.7, MTV: 0.5 ml vs. 1.0 ml and TLG: 1.0 ml vs. 3.0 ml).
Conclusion: TB and SAFOV PET/CT showed high diagnostic accuracy indices for N-staging in NSCLC patients. Sensitivity and PPV on TB PET/CT were slightly higher, compared to SAFOV PET/CT without statistical significance. However, TB PET/CT showed lower rate of incorrect N-staging and lower semi-quantitative thresholds for the detection positive mediastinal lymph nodes. Therefore, TB PET/CT might be advantageous in detecting small and low [18F]FDG-avidity mediastinal lymph node metastases in NSCLC patients.
Keywords: Lung cancer; N-staging; SAFOV PET; Total-body PET; [18F]FDG.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This study was approved by the UC Davis institutional review board (IRB 1506448). Written informed consent for inclusion was obtained. The study was performed in accordance with the Declaration of Helsinki. Conflict of interest: AR has received research support and speaker honoraria from Siemens and is an editor of this journal. LN is principal investigator of a service agreement with United Imaging Healthcare. LN is site PI of clinical trials supported by Novartis Pharmaceuticals Corporation. LN is PI of clinical trials supported by Telix Pharmaceuticals, Lantheus Medical Imaging and GE Healthcare. LN and RDB are PIs of a clinical trial supported by Lilly. RDB received research support from United Imaging Healthcare during this work. UC Davis has a revenue sharing agreement with United Imaging Healthcare. FS is PI of clinical research sponsored by Biogen. JWR has received consulting/advisory board fees from Boehringer Ingelheim, Daiichi Sankyo, Merck, EMD Serono, Roche/Genentech, BMS, Regeneron, Merus NV, Catalyst, Oncohost and Janssen and research funding to institution from AstraZeneca/MedImmune, Boehringer Ingelheim, Merck, Novartis, Revolution Medicines, Nuvalent, Summit, and Pfizer/SeaGen. All other authors have no conflicts of interest to report. RDB is PI on a study sponsored by Lilly.
Figures


References
-
- Crinò L, Weder W, van Meerbeeck J, Felip E. Early stage and locally advanced (non-metastatic) non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Annals Oncology: Official J Eur Soc Med Oncol. 2010;21(Suppl 5):v103–15. 10.1093/annonc/mdq207. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
