

Paracancerous binuclear hepatocytes assessed by computer program is a novel biomarker for short term recurrence of hepatocellular carcinoma after surgery
- PMID: 40113908
- PMCID: PMC11926264
- DOI: 10.1038/s41598-025-90004-4
Paracancerous binuclear hepatocytes assessed by computer program is a novel biomarker for short term recurrence of hepatocellular carcinoma after surgery
Abstract
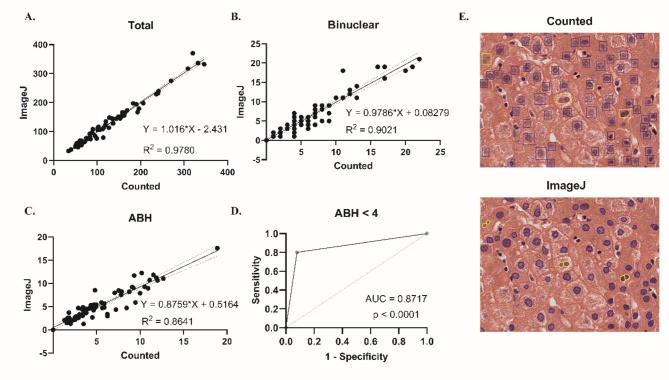
Hepatocellular carcinoma (HCC) is notorious for its high likelihood of recurrence even after radical surgery, which calls for effective adjuvant therapy based on more precise patient selection. The decline of the abundance of binuclear hepatocytes (ABH) in paracancerous liver tissues has been reported to indicate pathological changes in liver cells, leading to short-term recurrence within 2 years. In this research, we analyzed 34 HCC patients and 22 patients underwent liver surgery for non-HCC diseases. An ImageJ script was used to assess binuclear hepatocytes in the HE-staining specimens of paracancerous liver tissues. ABH significantly decreased in HCC patients and indicated poorer outcomes. Immunohistochemistry (IHC) assays suggested ploidy-related regulation of arginase 1 (ARG1) expression. Our findings suggested computer-assisted assessment of ABH as a possible biomarker for short-term HCC recurrence.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures




Similar articles
-
Attenuation of binuclear hepatocytes in the paracancerous liver tissue is associated with short-term recurrence of hepatocellular carcinoma post-radical surgery.FASEB J. 2023 Nov;37(11):e23271. doi: 10.1096/fj.202301219R. FASEB J. 2023. PMID: 37882195
-
Ascending E2F7a/b ratio facilitates KLF13 transcription in hepatocellular carcinoma and correlates with the abundance of binuclear hepatocytes (ABH) modulation for short-term recurrence.FASEB J. 2025 Mar 31;39(6):e70485. doi: 10.1096/fj.202402520R. FASEB J. 2025. PMID: 40116212 Free PMC article.
-
High expression of BBOX1 in paracancerous tissue is associated with poor prognosis in hepatocellular carcinoma patients.Sci Rep. 2024 Nov 18;14(1):28413. doi: 10.1038/s41598-024-78127-6. Sci Rep. 2024. PMID: 39557956 Free PMC article.
-
Gross appearance of hepatocellular carcinoma reflects E-cadherin expression and risk of early recurrence after surgical treatment.J Gastroenterol Hepatol. 2003 Jun;18(6):673-7. doi: 10.1046/j.1440-1746.2003.03021.x. J Gastroenterol Hepatol. 2003. PMID: 12753149
-
Suppression of SAMSN1 Expression is Associated with the Malignant Phenotype of Hepatocellular Carcinoma.Ann Surg Oncol. 2015 Dec;22 Suppl 3:S1453-60. doi: 10.1245/s10434-015-4524-1. Epub 2015 Mar 25. Ann Surg Oncol. 2015. PMID: 25805236
References
-
- Sung, H. et al. Global Cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.71(3), 209–249. 10.3322/caac.21660 (2021). - PubMed
-
- Tabrizian, P., Jibara, G., Shrager, B., Schwartz, M. & Roayaie, S. Recurrence of hepatocellular cancer after resection: Patterns, treatments, and prognosis. Ann. Surg.261(5), 947–955. 10.1097/sla.0000000000000710 (2015). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
