

Evaluation of immediate and sustained effects of transitioning quality long-acting reversible contraceptives (LARCs) services to public sector health facilities in Ghana: a pre-post intervention study
- PMID: 40114213
- PMCID: PMC11924747
- DOI: 10.1186/s12978-025-01979-2
Evaluation of immediate and sustained effects of transitioning quality long-acting reversible contraceptives (LARCs) services to public sector health facilities in Ghana: a pre-post intervention study
Abstract
Background: Long-acting reversible contraceptives (LARCs) are highly effective at preventing pregnancy and demonstrate favorable client satisfaction. However, limited knowledge, misconceptions, and concerns about side effects hinder LARC adoption. Marie Stopes International-Ghana collaborated with Ghana Health Service to implement a 5 year multifaceted intervention to transition quality LARC services from an outreach approach to being available in public sector health facilities. This study evaluates if the intervention resulted in immediate or sustained improvements in the provision of quality LARC services in the public sector.
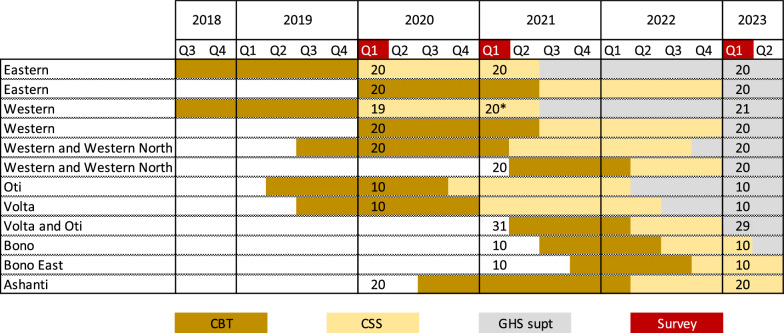
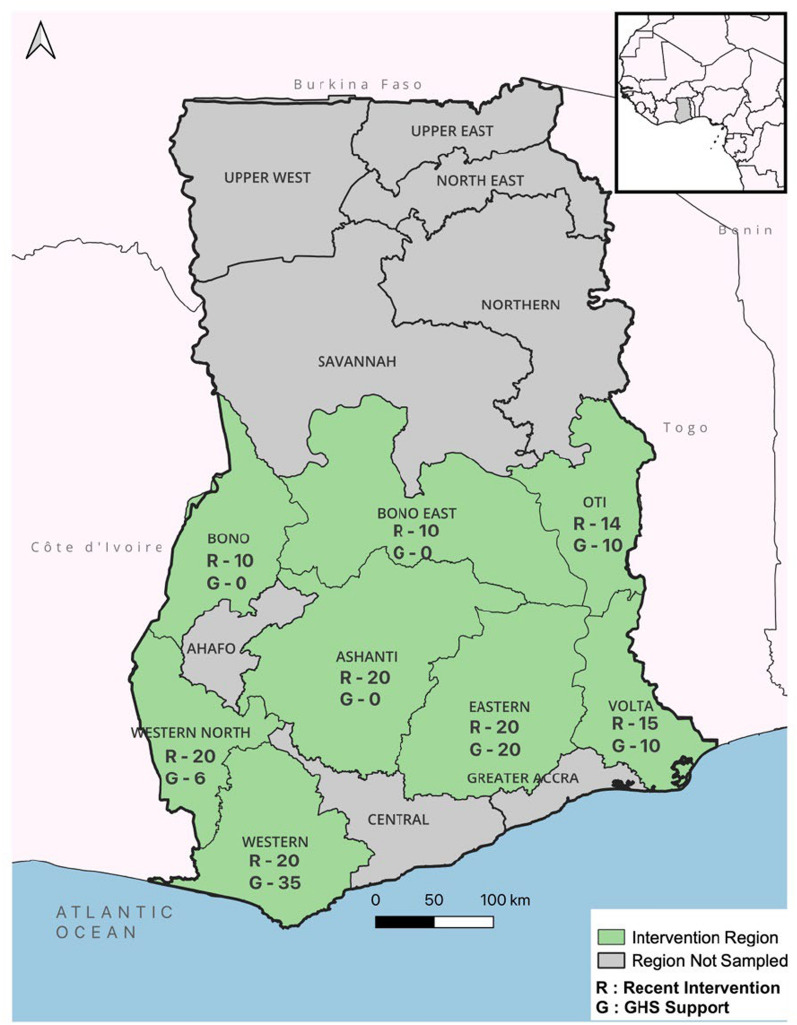
Methods: Using a pre-post intervention design, facility structural quality, providers' training, practice, and knowledge on the provision of LARCs, and clients' perceived service quality were assessed in 8 Ghanaian regions. Analyses compared endline and baseline data, categorized into two groups based on the program phase: Recent Intervention facilities and GHS Support facilities. Facility records on a 3 month volume of LARC provision were compared between the last quarters of 2019 and 2022. Multivariate logistic regressions of any increase in the volume of LARC provision were conducted with associated endline facility and provider characteristics summarized at the facility level.
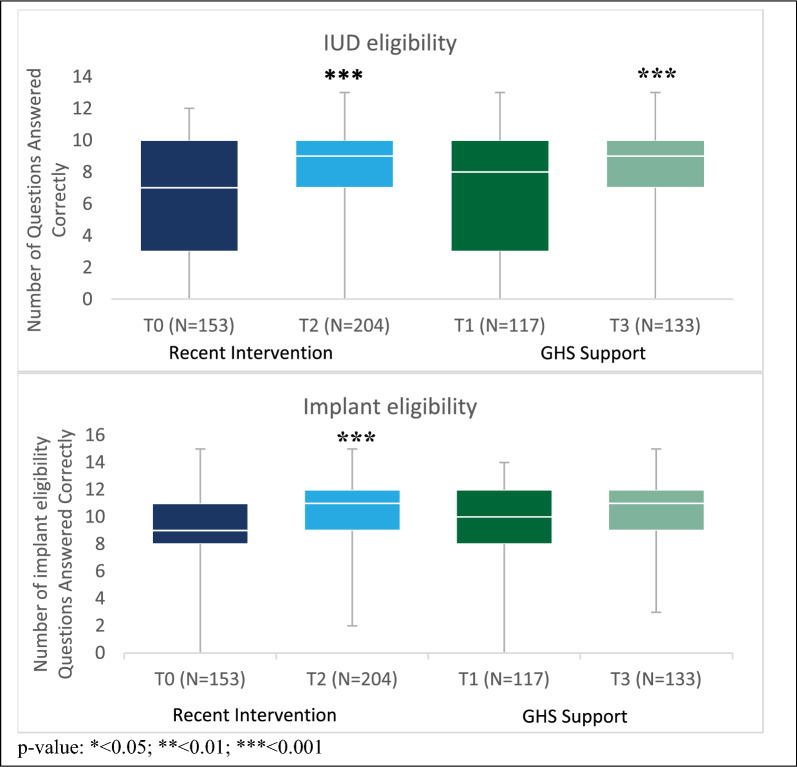
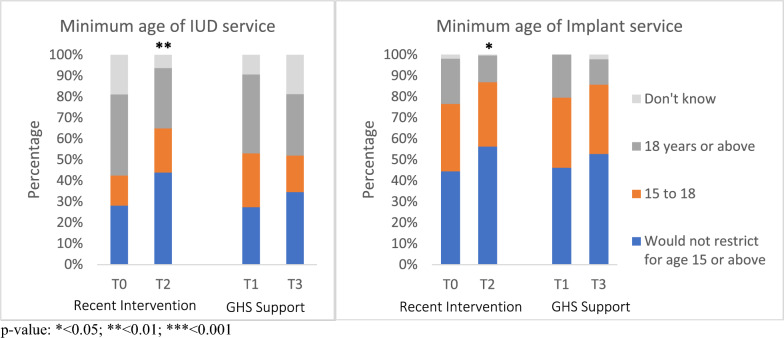
Results: Significant increases were found in the provision of IUD services among Recent Intervention facilities (CHPS facilities: T0 13%, T2 50%, p < 0.001; HC/Hospitals: T0 23%, T2 53%, p < 0.001), while almost all providers offered implant services across facility types and intervention phases. The proportion of providers ever been trained to insert LARCs increased. Immediate and sustained effects were found on knowledge of LARC provision. Although facilities had significant increases in usual IUD availability among those in Recent Intervention (CHPS: T0 13.0%, T2 50.0%, p < 0.001), availability of IUD decreased to pre-intervention level upon transition to GHS Support. Controlling for other factors, facilities which had transitioned to GHS support were far less likely than those in the Recent Intervention phase to have an increase in the volume of LARC provision.
Conclusions: This 5 year collaboration between MSI-Ghana and the Ghana Health Service increased the capacity of providers at 210 GHS facilities to provide high-quality LARC services. Future programs to improve LARC provision in the public sector may also consider including sustainable interventions to strengthen logistical management systems and targeting barriers to LARC access in the community. Increasing access to and use of modern contraception reduces unintended pregnancies and unsafe abortions, thereby decreasing maternal morbidity and mortality. Despite long-acting reversible contraceptives (LARCs) are highly effective at pregnancy prevention and favored by clients, utilization in many low- and middle-income countries has been low. In Ghana, less than half of women who want to delay, space, or limit childbearing use a modern contraceptive method. As the public sector is the predominant source of family planning services, improving the quality and provision of LARC services in the public sector has the most potential to increase women's access to LARCs. Marie Stopes International-Ghana collaborated with Ghana Health Service to implement a 5-year program to transition the provision of quality LARC services from its mobile clinic outreach model to public sector health facilities through a phased approach. We studied the immediate and longer-term effects on the provision and utilization of quality LARC services in the public sector. We collected three rounds of data from intervention facilities, associated providers, and clients. We found increased providers providing IUD services, trained in LARC provision, and increased and sustained knowledge needed for quality LARC services provision. Despite improvement, after the intervention ended, IUD availability at the facility decreased. Facilities that completed the intervention for at least several months were less likely to maintain the increased level of LARC provision than those still in the intervention or recently concluded. These findings underline the need for additional efforts to strengthen logistical management systems to ensure consistent provision of quality LARC services.
Keywords: Ghana; Long-acting reversible contraceptives; Multifaceted intervention; Public sector; Service quality; Sustained effects.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: All components of data collection were approved by ethical review committee in Ghana Health Service (reference number GHS-ERC016/10/19). Informed written consent was obtained from each participant. Participants were informed about their right to withdraw from participation during the informed consent process. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

Similar articles
-
Magnitude and factors for method discontinuation and switching among long acting reversible contraceptive users in health facilities of Southern Ethiopia.Reprod Health. 2022 Feb 19;19(1):47. doi: 10.1186/s12978-022-01357-2. Reprod Health. 2022. PMID: 35183214 Free PMC article.
-
Strengthening systems to provide long-acting reversible contraceptives (LARCs) in public sector health facilities in Uganda and Zambia: Program results and learnings.PLoS One. 2023 Aug 18;18(8):e0290115. doi: 10.1371/journal.pone.0290115. eCollection 2023. PLoS One. 2023. PMID: 37594954 Free PMC article.
-
Mentoring, Task Sharing, and Community Outreach Through the TutoratPlus Approach: Increasing Use of Long-Acting Reversible Contraceptives in Senegal.Glob Health Sci Pract. 2016 Aug 18;4 Suppl 2(Suppl 2):S33-43. doi: 10.9745/GHSP-D-15-00328. Print 2016 Aug 11. Glob Health Sci Pract. 2016. PMID: 27540123 Free PMC article.
-
Barriers and facilitators of acceptability and uptake of long-acting reversible contraceptives in Ethiopia: a systematic review using the COM-B model.Syst Rev. 2025 May 3;14(1):99. doi: 10.1186/s13643-025-02827-x. Syst Rev. 2025. PMID: 40319326 Free PMC article.
-
Accessibility and uptake of modern contraceptive methods in Pakistan - a critical view on what works?J Pak Med Assoc. 2021 Nov;71(Suppl 7)(11):S20-S32. J Pak Med Assoc. 2021. PMID: 34793425 Review.
References
-
- Stover J, Ross J. How increased contraceptive use has reduced maternal mortality. Matern Child Health J. 2010;14(5):687–95. - PubMed
-
- Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet. 2012;380(9837):111–25. - PubMed
-
- Bahamondes L, Fernandes A, Monteiro I, Bahamondes MV. Long-acting reversible contraceptive (LARCs) methods. Best Pract Res Clin Obstet Gynaecol. 2020;66:28–40. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
