

Prognostic nomogram for synchronous metastatic nasopharyngeal carcinoma: a retrospective multicentre study
- PMID: 40114228
- PMCID: PMC11927208
- DOI: 10.1186/s13014-025-02602-1
Prognostic nomogram for synchronous metastatic nasopharyngeal carcinoma: a retrospective multicentre study
Abstract
Background: Patients with synchronous metastatic nasopharyngeal carcinoma (smNPC) exhibit significant heterogeneity, and clinical prognostic models suitable for this cohort remain limited. We aimed to develop a prognostic prediction tool to facilitate personalised prognostic assessments and inform treatment decisions for these patients.
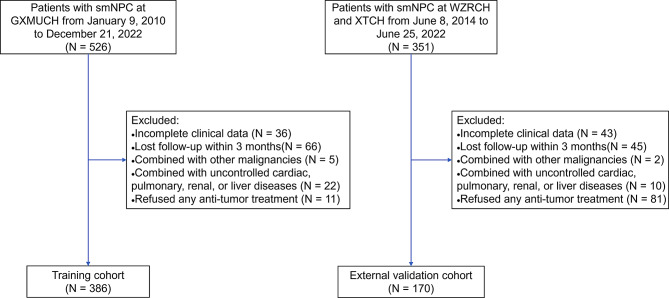
Methods: This retrospective multicentre study enrolled 556 patients with smNPC. The training cohort comprised 386 patients from Guangxi Medical University Cancer Hospital, while the external validation cohort comprised 170 patients from Wuzhou Red Cross Hospital and Xiangtan Central Hospital. We applied the Cox proportional hazards model to determine factors associated with overall survival (OS). A nomogram prognostic model was developed to predict OS based on the identified prognostic factors. The model's predictive performance was evaluated for discrimination and calibration, and patients were stratified based on their calculated prognostic risk scores. Kaplan-Meier survival curves were employed to assess prognostic differences across the stratified groups.
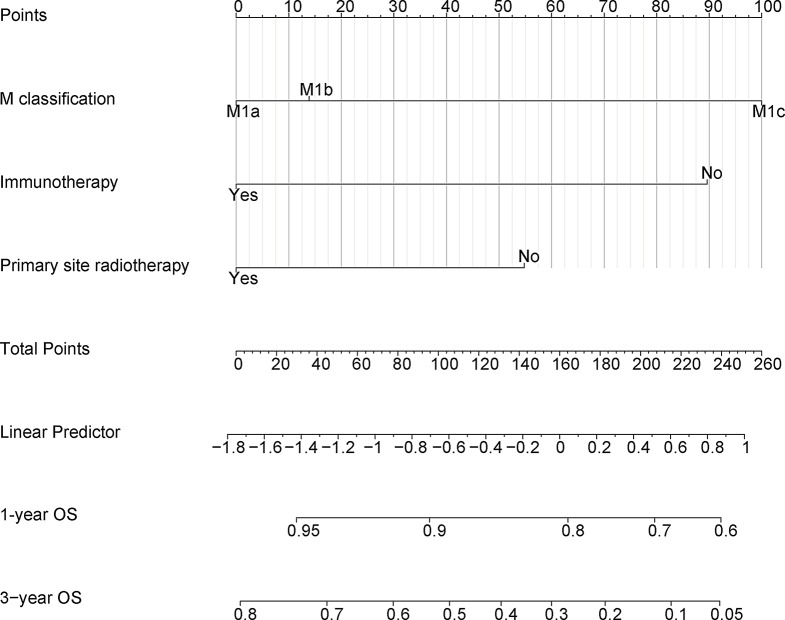
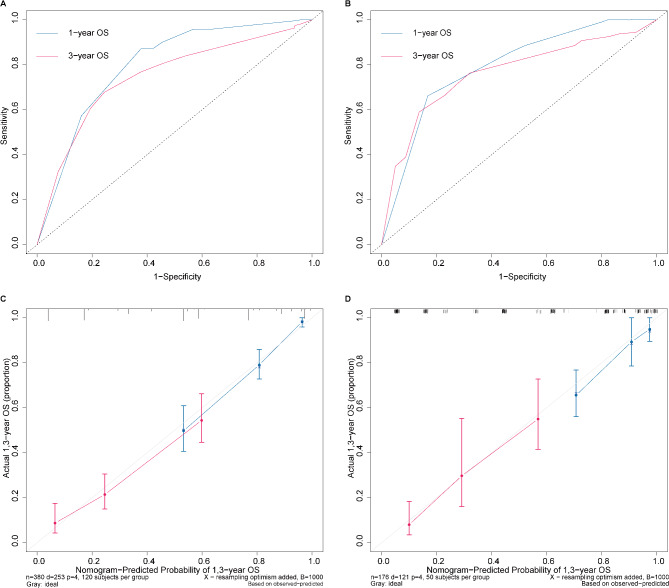
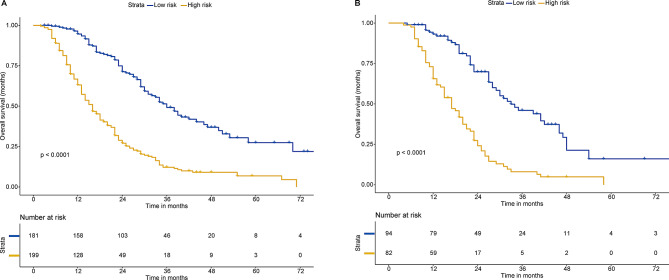
Results: Multivariate analysis identified that M classification, primary tumour radiotherapy, and immunotherapy were significantly associated with OS. A prognostic nomogram integrating these variables exhibited good discrimination (C-index: 0.743) and calibration, which was validated in an external validation cohort. Patients stratified by the model-derived risk scores into high- and low-risk groups showed a significant difference in survival disparity.
Conclusions: We established a nomogram prognostic model that effectively facilitated individualised prognostic prediction and risk stratification in patients with smNPC, thereby assisting clinicians in treatment decision-making.
Keywords: Multicentre study; Multimodality treatment; Nomogram; Synchronous metastasis nasopharyngeal carcinoma.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This multicentre study was approved by the Institutional Review Boards of Guangxi Medical University Cancer Hospital (GXMUCH), Xiangtan Central Hospital (XTCH), and Wuzhou Red Cross Hospital (WZRCH). Written informed consent was deemed unnecessary due to the study’s retrospective design. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Development and validation of a gene expression-based signature to predict distant metastasis in locoregionally advanced nasopharyngeal carcinoma: a retrospective, multicentre, cohort study.Lancet Oncol. 2018 Mar;19(3):382-393. doi: 10.1016/S1470-2045(18)30080-9. Epub 2018 Feb 7. Lancet Oncol. 2018. PMID: 29428165
-
Establishment and Validation of a Nomogram for Nasopharyngeal Carcinoma Patients Concerning the Prognostic Effect of Parotid Lymph Node Metastases.Cancer Res Treat. 2020 Jul;52(3):855-866. doi: 10.4143/crt.2019.772. Epub 2020 Mar 10. Cancer Res Treat. 2020. PMID: 32164051 Free PMC article.
-
A nomogram based on circulating CD8+ T cell and platelet-to-lymphocyte ratio to predict overall survival of patients with locally advanced nasopharyngeal carcinoma.Radiat Oncol. 2024 Aug 13;19(1):108. doi: 10.1186/s13014-024-02500-y. Radiat Oncol. 2024. PMID: 39138513 Free PMC article.
-
Prognostic value of tumour-stroma ratio in nasopharyngeal carcinoma: a two-center retrospective study.Radiat Oncol. 2025 May 23;20(1):87. doi: 10.1186/s13014-025-02627-6. Radiat Oncol. 2025. PMID: 40410801 Free PMC article.
-
A novel prognostic model predicts overall survival in patients with nasopharyngeal carcinoma based on clinical features and blood biomarkers.Cancer Med. 2021 Jun;10(11):3511-3523. doi: 10.1002/cam4.3839. Epub 2021 May 11. Cancer Med. 2021. PMID: 33973727 Free PMC article.
References
-
- Chen Y-P, Chan ATC, Le Q-T, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394:64–80. - PubMed
-
- Zou X, You R, Liu H, He Y-X, Xie G-F, Xie Z-H, et al. Establishment and validation of M1 stage subdivisions for de novo metastatic nasopharyngeal carcinoma to better predict prognosis and guide treatment. Eur J Cancer. 2017;77:117–26. - PubMed
-
- Lee V, Kwong D, Leung T-W, Lam K-O, Tong C-C, Lee A. Palliative systemic therapy for recurrent or metastatic nasopharyngeal carcinoma– how far have we achieved? Crit Rev Oncol/Hematol. 2017;114:13–23. - PubMed
-
- Chan SK, Lin C, Huang SH, Chau TC, Guo QJ, O’Sullivan B, et al. Refining TNM-8 M1 categories with anatomic subgroups for previously untreated de novo metastatic nasopharyngeal carcinoma. Oral Oncol. 2022;126:105736. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
