

Predictors of preterm births in North Dakota: a retrospective study of the North Dakota Pregnancy Risk Assessment Monitoring System (PRAMS)
- PMID: 40115276
- PMCID: PMC11925044
- DOI: 10.7717/peerj.19049
Predictors of preterm births in North Dakota: a retrospective study of the North Dakota Pregnancy Risk Assessment Monitoring System (PRAMS)
Abstract
Background: Preterm births represent approximately 10% of all births in the United States (US) annually. Although North Dakota (ND) has large rural and American Indian populations that experience disparities in health outcomes relative to the general population, few studies have investigated risk factors of preterm births in this state. Therefore, the objective of this study was to investigate predictors of preterm births in ND among women who had a live singleton birth and no prior history of preterm births.
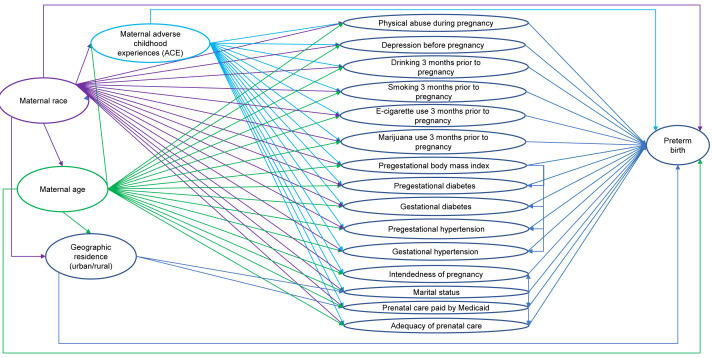
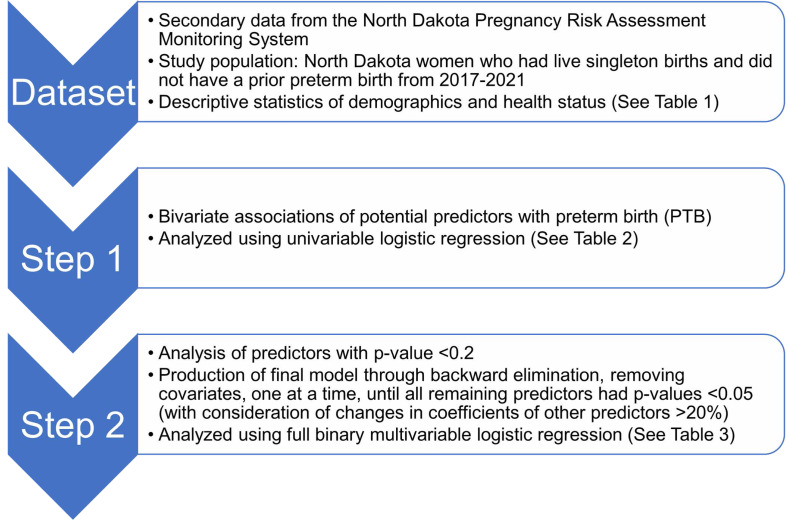
Methods: Data on live births from 2017 to 2021 were obtained from the ND Pregnancy Risk Assessment Monitoring System. Potential predictors of preterm birth were identified using a conceptual model. Multivariable logistic regression was then used to investigate and identify significant predictors of preterm births.
Results: The overall prevalence of preterm birth in North Dakota from 2017 to 2021 was 8.1%. However, among the population of interest in this study, which excluded births with multiple infants as well as women with a prior history of preterm birth, the preterm birth rate was 6.4%. Race, age, pregestational diabetes, and gestational hypertension were significantly associated with preterm birth in the final multivariable logistic model. The odds of preterm birth were higher among women who were American Indian (adjusted odds ratio (AOR) = 1.7, 95% confidence interval (CI) [1.3-2.4]), were aged 35 years or older (AOR = 1.6, 95% CI [1.01-2.5]), had pregestational diabetes (AOR = 4.3, 95% CI [2.0-9.3]), and had gestational hypertension (AOR = 4.5, 95% CI [3.1-6.7]) compared to women who were White, aged 20-34 years, and did not have pregestational diabetes or gestational hypertension.
Conclusions: Preventing and controlling chronic diabetes and hypertensive disorders of pregnancy is critical for reducing the risk of preterm birth, especially among women of advanced maternal age. Further research is needed to understand the underlying causes of racial disparities of preterm birth in ND.
Keywords: Logistic regression; North Dakota; PRAMS; Pregnancy Risk Assessment Monitoring; Preterm birth; United States.
©2025 Njau et al.
Conflict of interest statement
Agricola Odoi is an Academic Editor for PeerJ.
Figures
Similar articles
-
The Association Between Diabetes Mellitus Among American Indian/Alaska Native Populations with Preterm Birth in Eight US States from 2004-2011.Matern Child Health J. 2015 Nov;19(11):2419-28. doi: 10.1007/s10995-015-1761-7. Matern Child Health J. 2015. PMID: 26112750
-
The Impact of Maternal Diabetes, Obesity and Race on Infant Birth Weights in South Dakota.S D Med. 2017 Feb;70(2):61-66. S D Med. 2017. PMID: 28810088
-
Disparities in Risk Factors and Birth Outcomes Among American Indians in North Dakota.Matern Child Health J. 2018 Oct;22(10):1519-1525. doi: 10.1007/s10995-018-2551-9. Matern Child Health J. 2018. PMID: 29936660
-
Race and ethnic disparities in fetal mortality, preterm birth, and infant mortality in the United States: an overview.Semin Perinatol. 2011 Aug;35(4):200-8. doi: 10.1053/j.semperi.2011.02.017. Semin Perinatol. 2011. PMID: 21798400 Review.
-
Predictors of Inflammation-Mediated Preterm Birth.Physiology (Bethesda). 2025 Jan 1;40(1):0. doi: 10.1152/physiol.00022.2024. Epub 2024 Aug 6. Physiology (Bethesda). 2025. PMID: 39106300 Free PMC article. Review.
References
-
- American Academy of Pediatrics . Adverse childhood experiences and the lifelong consequences of trauma. Itasca: American Academy of Pediatrics; 2014.
MeSH terms
LinkOut - more resources
Full Text Sources
