

Comparison of the Pediatric Sequential Organ Failure Assessment (p SOFA) Score and Lactate Clearance as Predictors of Morbidity and Mortality in Pediatric Sepsis: A Prospective Observational Study
- PMID: 40115724
- PMCID: PMC11923480
- DOI: 10.7759/cureus.79172
Comparison of the Pediatric Sequential Organ Failure Assessment (p SOFA) Score and Lactate Clearance as Predictors of Morbidity and Mortality in Pediatric Sepsis: A Prospective Observational Study
Abstract
Background: Sepsis continues to be a leading cause of illness and mortality in children around the world. Various scoring systems have been devised to predict the outcome of pediatric sepsis. Pediatric sequential organ failure assessment (p SOFA) and lactate clearance are the two commonly used methods.
Objective: The aim of this study was to compare the p SOFA score with lactate clearance as predictors of morbidity and mortality in pediatric sepsis, to compare the initial plasma lactate level and lactate clearance, and to know which is better to predict outcomes in sepsis and septic shock.
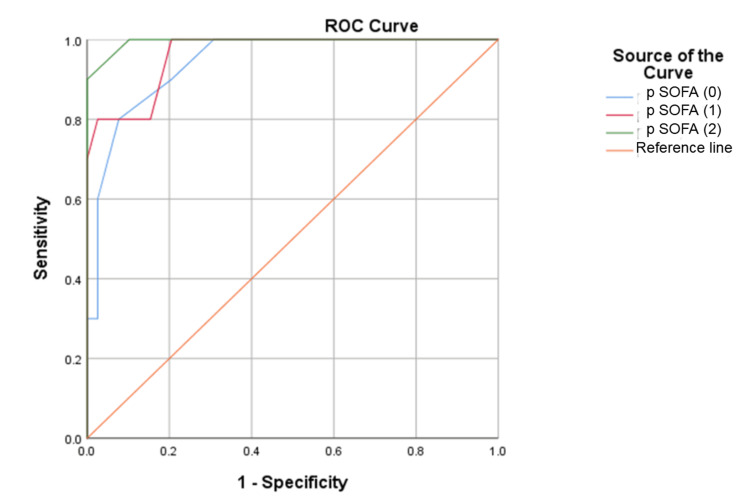
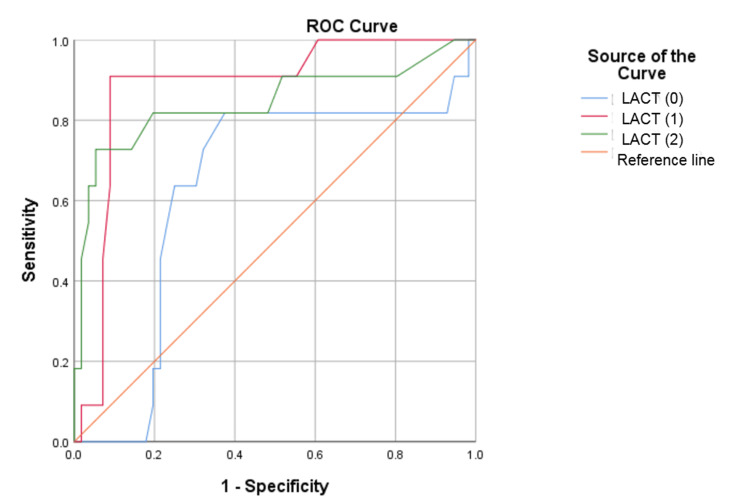
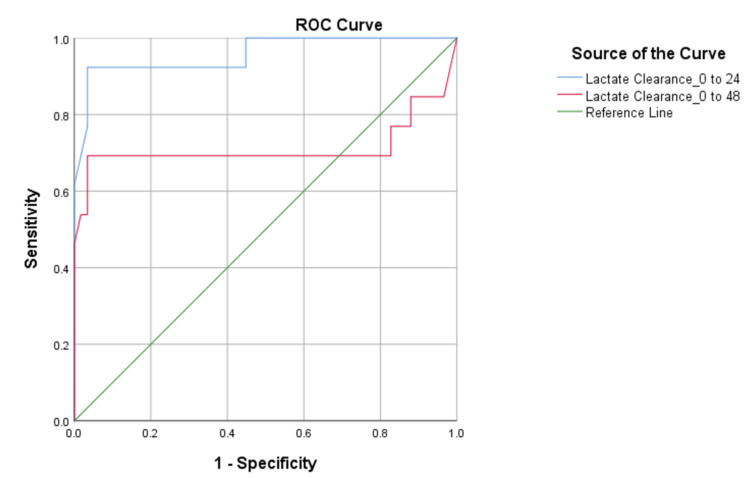
Methods: This prospective observational study was conducted in a pediatric intensive care unit of a tertiary care teaching hospital from July 2022 to June 2024. The blood lactate level and p SOFA score were assessed at admission and at 24 and 48 hours, and lactate clearance was calculated at 24 and 48 hours of admission. The receiver operating characteristic (ROC) curve was plotted to predict deaths using p SOFA, lactate level, and lactate clearance.
Results: A total of 71 children were enrolled in the study. All children were divided into two groups, 58 (82%) survivors and 13 (18%) non-survivors. The most common diagnosis was pneumonia, observed in 31 (43.6%) children. Compared to survivors, non-survivors had a higher prevalence of multiple organ dysfunction syndrome (MODS). The most common organ system involved was the cardiovascular, in 50 (70%) cases. For predicting mortality, p SOFA scores were statistically significant at admission and at 24 and 48 hours with a high area under the curve (AUC) at 48 hours (0.985). Lactate clearance at 24 hours was a better predictor of mortality than at 48 hours with a higher AUC (0.958).
Conclusion: Both p SOFA score at 48 hours and lactate clearance at 24 hours were significant predictors of mortality. Among both parameters, lactate clearance at 24 hours was superior in predicting mortality early.
Keywords: lactate clearance; mortality; p sofa; pediatric sepsis; picu; septic shock.
Copyright © 2025, Aggarwal et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Institutional Ethics Committee, Kalinga Institute of Medical Sciences issued approval KIIT/KIMS/IEC/985/2022. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Sequential Organ Failure Assessment Score As a Predictor of Outcome in Sepsis in Pediatric Intensive Care Unit.J Pediatr Intensive Care. 2021 Jun;10(2):110-117. doi: 10.1055/s-0040-1714705. Epub 2020 Jul 30. J Pediatr Intensive Care. 2021. PMID: 33884211 Free PMC article.
-
The Value of the Sequential Organ Failure Assessment (SOFA) Score and Serum Lactate Level in Sepsis and Its Use in Predicting Mortality.Cureus. 2023 Jul 30;15(7):e42683. doi: 10.7759/cureus.42683. eCollection 2023 Jul. Cureus. 2023. PMID: 37649942 Free PMC article.
-
[Lactic acid, lactate clearance and procalcitonin in assessing the severity and predicting prognosis in sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Apr;32(4):449-453. doi: 10.3760/cma.j.cn121430-20200129-00086. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32527351 Chinese.
-
[Comparison of four scoring systems for predicting ICU mortality in patients with sepsis].Nan Fang Yi Ke Da Xue Xue Bao. 2020 Apr 30;40(4):513-518. doi: 10.12122/j.issn.1673-4254.2020.04.10. Nan Fang Yi Ke Da Xue Xue Bao. 2020. PMID: 32895135 Free PMC article. Chinese.
-
Lactate, an Essential Metabolic Marker in the Diagnosis and Management of Pediatric Conditions.Diagnostics (Basel). 2025 Mar 23;15(7):816. doi: 10.3390/diagnostics15070816. Diagnostics (Basel). 2025. PMID: 40218166 Free PMC article. Review.
References
-
- Reducing the global burden of sepsis in infants and children: a clinical practice research agenda. Carcillo JA. Pediatr Crit Care Med. 2005;6:0–64. - PubMed
-
- WHO estimates of the causes of death in children. Bryce J, Boschi-Pinto C, Shibuya K, Black RE, The WHO Child Health Epidemiology Reference Group. The Lancet. 2005;365:1147–1152. - PubMed
LinkOut - more resources
Full Text Sources