

Claudin 18 (43-14A clone) expression in pancreatic ductal adenocarcinoma: Assessment of a potential clinical biomarker for zolbetuximab therapy
- PMID: 40117781
- PMCID: PMC11979426
- DOI: 10.1016/j.tranon.2025.102362
Claudin 18 (43-14A clone) expression in pancreatic ductal adenocarcinoma: Assessment of a potential clinical biomarker for zolbetuximab therapy
Abstract
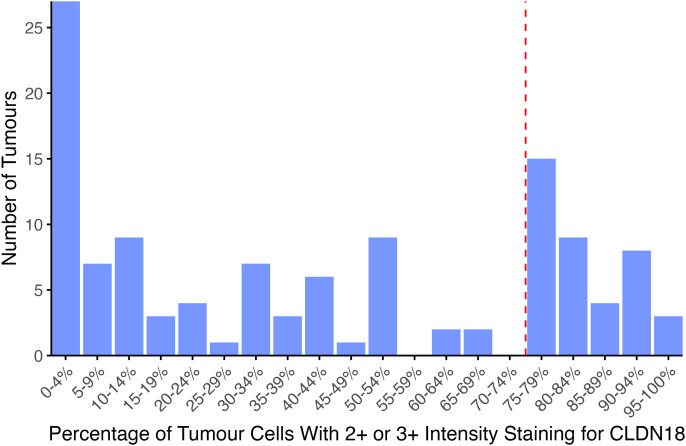
Pancreatic ductal adenocarcinoma (PDAC) remains highly lethal, with a five-year survival rate below 15 %. Claudin 18.2 (CLDN18.2) has emerged as a novel potential therapeutic target in PDAC. Zolbetuximab, a monoclonal antibody targeting CLDN18.2, has demonstrated therapeutic benefit in gastric cancers and is now in phase 2 clinical trials for PDAC. Trial eligibility for zolbetuximab requires tumor membranous immunohistochemical staining with the pan-claudin 18 companion diagnostic antibody clone 43-14A. However, the expression of CLDN18 detected using this clone has only been evaluated in 62 patients from a single retrospective study. Herein, we report immunohistochemical staining using 43-14A on surgically resected PDAC samples (n = 120). Samples were stained following the protocol used in clinical trials, using the 43-14A VENTANA antibody in a prediluted kit, and according to the manufacturer's recommended protocol. Positive cases were defined as ≥ 75 % of tumor cells exhibiting membranous staining with an intensity of ≥ 2+. Out of 120 PDAC cases, 39 (32.5 %) stained positive for CLDN18 with 43-14A. A significant association was observed between lower tumor grade and higher 43-14A staining (p < 0.05). CLDN18-positive cases demonstrated significantly improved survival at the cohort's median overall survival (23 months, p < 0.05), suggesting that claudin expression could serve as a both a diagnostic and prognostic marker. Our findings indicate that 32.5 % of PDAC tumors in this cohort are positive for CLDN18, suggesting that a significant proportion of patients with PDAC could benefit from zolbetuximab and other CLDN18.2 targeted immunotherapies if pancreatic cancer therapeutic trials prove successful.
Keywords: 43–14a; Biomarkers; Claudin 18 protein, human; Immunohistochemistry; Pancreatic ductal carcinoma; zolbetuximab.
Copyright © 2025. Published by Elsevier Inc.
Conflict of interest statement
Declaration of competing interest Dr. Arnason has received honoraria from Astellas Pharmaceuticals for participation in a Canadian upper gastrointestinal cancer biomarker guideline advisory committee. Dr. Ramjeesingh has received honoraria from Roche for advisory boards. The investigators in this study received a free claudin 18 (43–14A) kit from Roche.
Figures




References
-
- Abidoye O., Cho Y.M., Bhushan S., Adewunmi C., Choudhury H. Trends in pancreatic cancer incidence and mortality in the United States from 2000 to 2019; a SEER based study. Published online January 5, 2023. doi:10.12688/f1000research.122872.1. - DOI
-
- Canadian cancer statistics advisory in collaboration with the Canadian cancer society, statistics Canada and the public health agency of Canada. Canadian Cancer Stat. 2022 Published online.
LinkOut - more resources
Full Text Sources
