

Current Drug Treatment for Acute and Recurrent Pericarditis
- PMID: 40119189
- PMCID: PMC12031812
- DOI: 10.1007/s40265-025-02169-x
Current Drug Treatment for Acute and Recurrent Pericarditis
Abstract
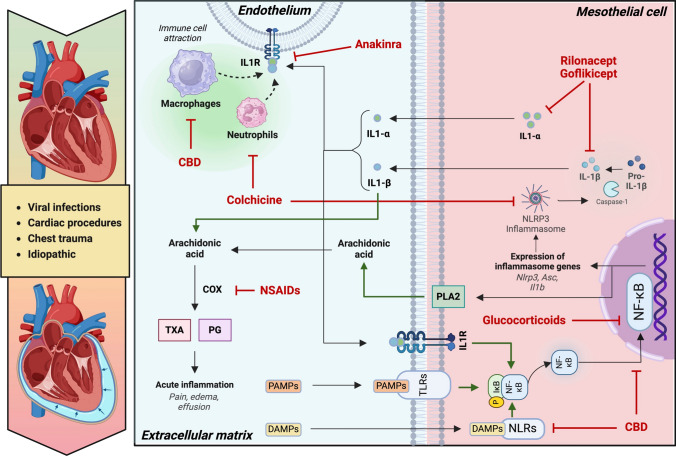
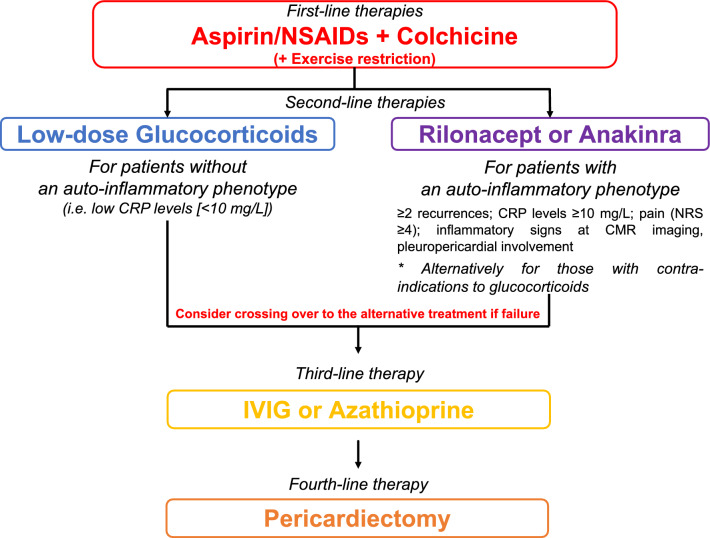
Pericarditis is the most frequent pericardial disease and presents with a relatively benign course when treated according to guideline-directed therapies at first presentation. Recurrence is the most frequent complication and may occur more frequently after a first episode, in patients with autoimmune etiology, in patients who received glucocorticoids, or after rapid (i.e., within 1 month) tapering of anti-inflammatory drugs. The therapeutic armamentarium for pericarditis includes high-dose nonsteroidal anti-inflammatory drugs (NSAIDs) that are tapered rapidly once symptoms are controlled. Colchicine is necessary to both relieve symptoms and reduce the rate of recurrences and is continued for at least 3-6 months. Low- to moderate-dose glucocorticoids are reserved for patients with a first recurrence for which NSAIDs and colchicine failed and/or who have an autoimmune disorder, with a slow tapering. Interleukin-1 blockers-anakinra, rilonacept, and goflikicept-are used as a third-line option in patients who cannot come off glucocorticoids or as second-line therapy after NSAIDs and colchicine in patients with contraindications to glucocorticoids or in those with high-risk features (i.e., multiple episodes, markedly elevated inflammatory markers, or extensive abnormalities at pericardial imaging) in whom treatment with glucocorticoids is unlikely to succeed.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Funding: The study received no funding. Conflicts of interest: AA has served as a consultant for Kiniksa, Novo Nordisk, and Monte Rosa Therapeutics. All the other authors have nothing to disclose. Ethics approval: Not applicable. Consent to participate: Not applicable. Consent for publication: Not applicable. Availability of data and material: Not applicable. Code availability: Not applicable. Author contributions: AB and AA conceived the general structure of the manuscript. AB, DS, and AA drafted the first version of the manuscript. DS drafted Fig. 1. AA critically revised the manuscript. All authors read and approved the final version of the manuscript.
Figures
References
-
- Adler Y, Charron P, Imazio M, Badano L, Baron-Esquivias G, Bogaert J, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) Endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36:2921–64. - PMC - PubMed
-
- Cremer PC, Klein AL, Imazio M. Diagnosis, risk stratification, and treatment of pericarditis: a review. JAMA. 2024;332:1090–100. - PubMed
-
- Chiabrando JG, Bonaventura A, Vecchie A, Wohlford GF, Mauro AG, Jordan JH, et al. Management of acute and recurrent pericarditis: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75:76–92. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
