Safety of sulfamethoxazole-trimethoprim for the treatment of bacterial infection in outpatient settings: A systematic review and meta-analysis with active comparator disproportionality analysis
- PMID: 40129122
- PMCID: PMC12272531
- DOI: 10.1002/bcp.70051
Safety of sulfamethoxazole-trimethoprim for the treatment of bacterial infection in outpatient settings: A systematic review and meta-analysis with active comparator disproportionality analysis
Abstract
Aims: Sulfamethoxazole-trimethoprim (SMX-TMP) is a widely used antibiotic for treating bacterial infections, but its safety in adult outpatients remains understudied. This systematic review and meta-analysis evaluated the safety profile of SMX-TMP and identified critical research gaps. The pharmacovigilance study aimed to validate and extend findings from meta-analyses to better understand the real-world safety of SMX-TMP.
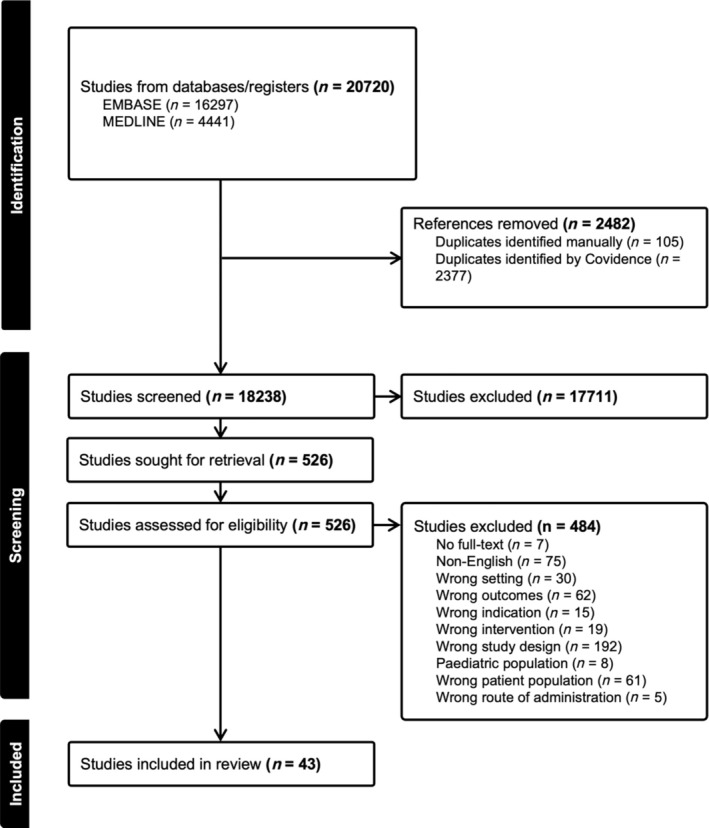
Methods: We searched MEDLINE and Embase up to 12 August 2024, to identify studies comparing adverse drug events (ADEs) following SMX-TMP vs. other antibiotics in adult outpatients. Meta-analyses were performed where data allowed. A pharmacovigilance study using the Food and Drug Administration Adverse Event Reporting System was conducted to supplement our findings.
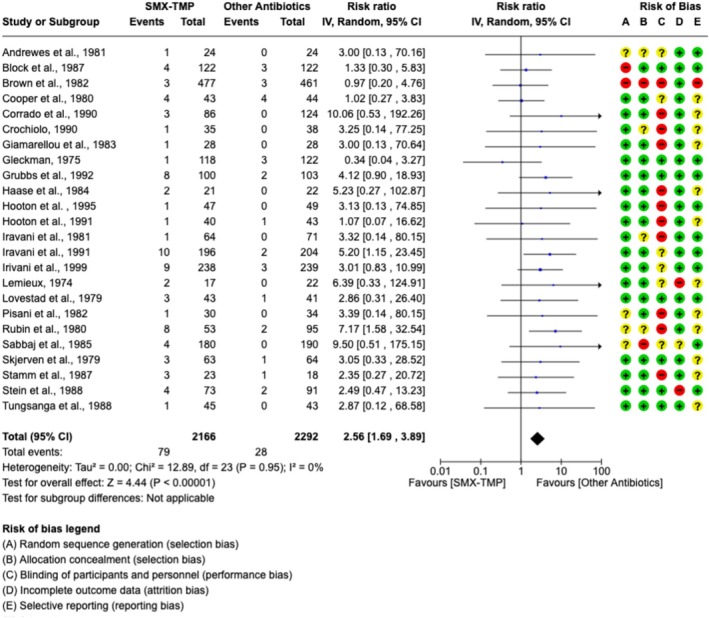
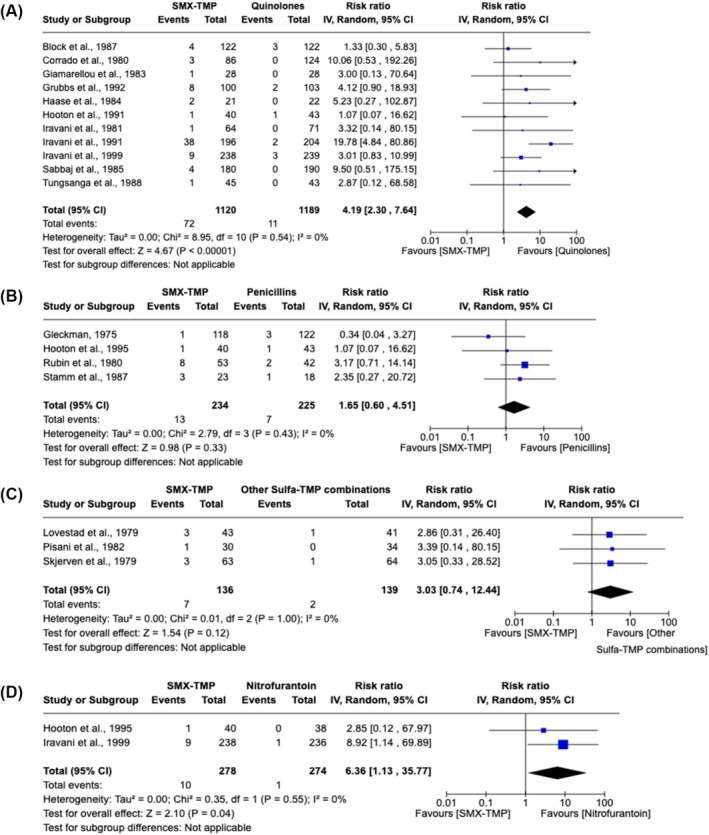
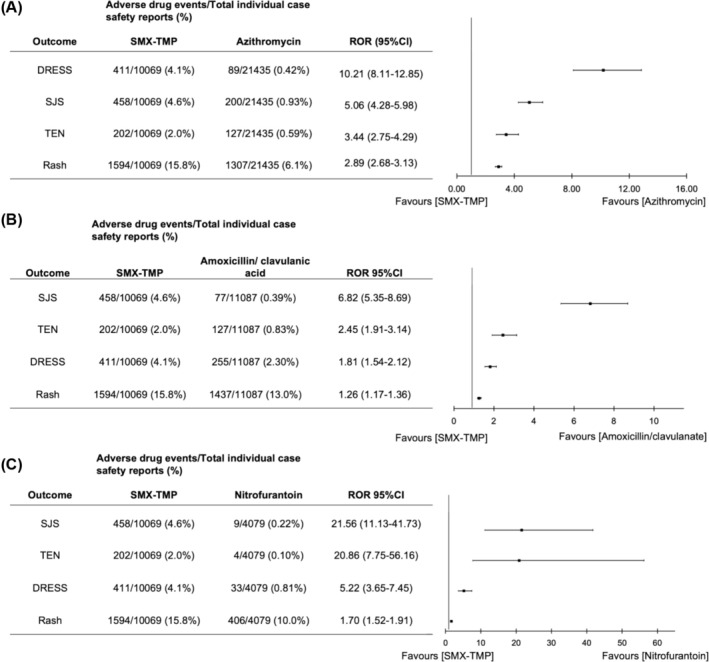
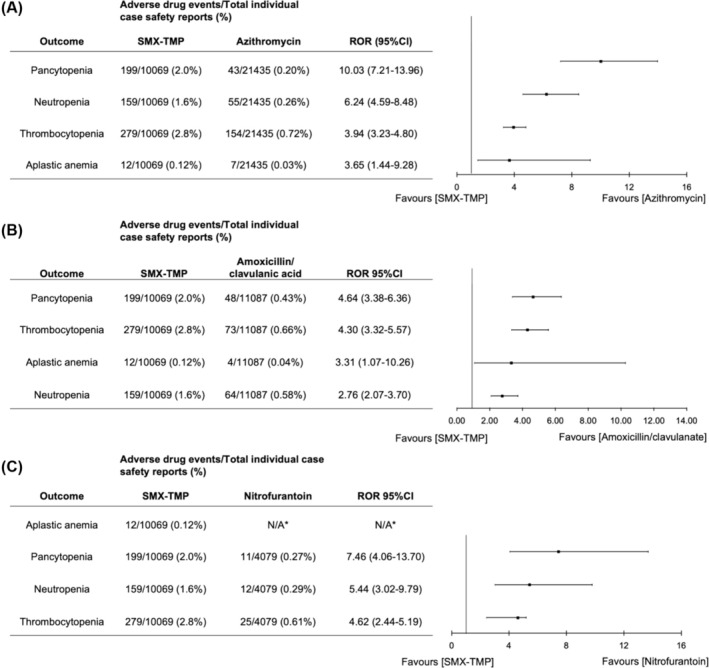
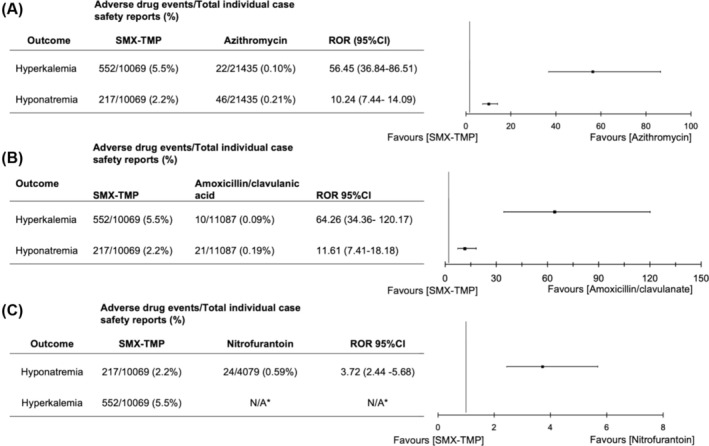
Results: Our review, which included 43 studies, found SMX-TMP had a nearly 3-fold higher risk of rash compared to other antibiotics (pooled risk ratio 2.56, 95% confidence interval [1.69, 3.89], I2 = 0%, n = 4458 participants, 24 randomized control trials). Pharmacovigilance data confirmed a higher frequencies of skin disorders and other ADEs compared to various comparator drugs. Compared to azithromycin, SMX-TMP was associated with a 5-fold increase in Stevens-Johnson syndrome, a 3-fold increase in toxic epidermal necrolysis, and a 10-fold increase in drug reaction with eosinophilia and systemic symptoms. Additionally, SMX-TMP showed a 10-fold increase in reports of pancytopenia, a 6-fold increase in neutropenia, a 4-fold increase in both thrombocytopenia and aplastic anaemia, a 56-fold increase in hyperkalaemia, and a 10-fold increase in hyponatraemia.
Conclusion: Our meta-analyses and pharmacovigilance study suggested SMX-TMP was associated with increased risk of ADEs compared to other antibiotics including amoxicillin/clavulanate, azithromycin and nitrofurantoin. Further robust research is essential to confirm these safety signals and guide clinical practice.
Keywords: Septra; adverse drug event; cotrimoxazole; cutaneous drug reaction.
© 2025 The Author(s). British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Conflict of interest statement
All authors reported no conflicts of interest.
Figures
Similar articles
-
Safety of sulfamethoxazole-trimethoprim for the treatment of bacterial infection in outpatient settings: A systematic review and meta-analysis with active comparator disproportionality analysis.Br J Clin Pharmacol. 2025 Jun;91(6):1632-1648. doi: 10.1111/bcp.70051. Br J Clin Pharmacol. 2025. PMID: 40441678 Free PMC article.
-
Severe Acute Respiratory Failure Associated With Trimethoprim/Sulfamethoxazole Among Adolescent and Young Adults: An Active Comparator-Restricted Disproportionality Analysis From the FDA Adverse Event Reporting System (FAERS) Database.Ann Pharmacother. 2025 Oct;59(10):904-911. doi: 10.1177/10600280251320690. Epub 2025 Feb 26. Ann Pharmacother. 2025. PMID: 40012193
-
Human Leukocyte Antigens and Sulfamethoxazole/Cotrimoxazole-Induced Severe Cutaneous Adverse Reactions: A Systematic Review and Meta-Analysis.JAMA Dermatol. 2024 May 1;160(5):525-534. doi: 10.1001/jamadermatol.2024.0210. JAMA Dermatol. 2024. PMID: 38568509 Free PMC article.
-
Comparative efficacy and safety of treatment regimens for Pneumocystis jirovecii pneumonia in people living with HIV: a systematic review and network meta-analysis of randomized controlled trials.Clin Microbiol Infect. 2025 May;31(5):713-723. doi: 10.1016/j.cmi.2024.12.024. Epub 2024 Dec 26. Clin Microbiol Infect. 2025. PMID: 39732393
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical