

Impact of Age and Factor Xa Inhibitor Concentrations on Bleeding Risk in Patients with Atrial Fibrillation
- PMID: 40129295
- PMCID: PMC12166260
- DOI: 10.1002/cpt.3654
Impact of Age and Factor Xa Inhibitor Concentrations on Bleeding Risk in Patients with Atrial Fibrillation
Abstract
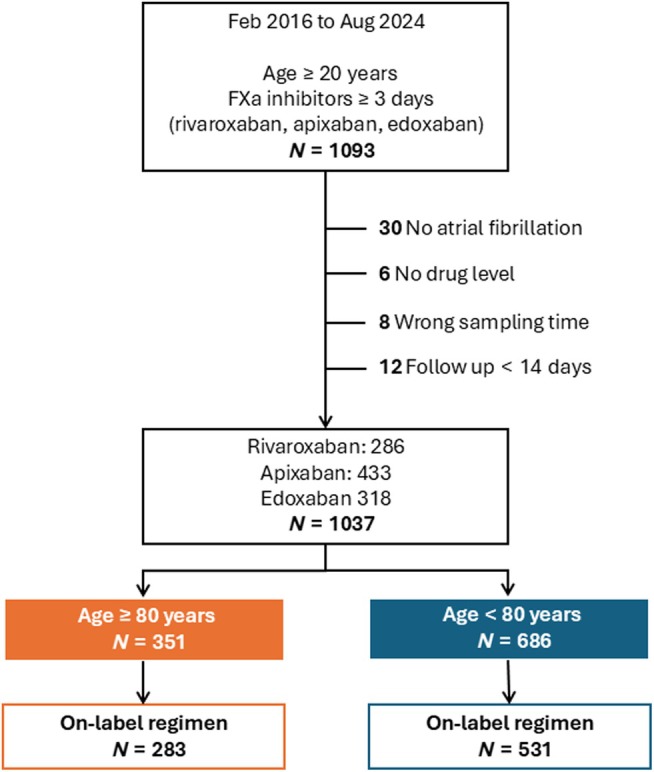
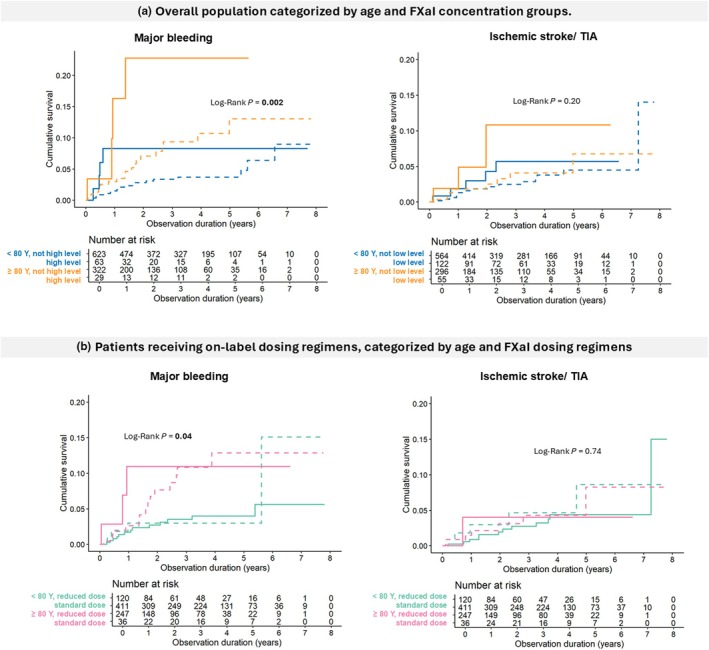
This study aimed to analyze differences in the exposure-response relationship for factor Xa inhibitors (FXaI) between patients aged ≥ 80 and < 80 years. Patients with atrial fibrillation (AF) taking rivaroxaban, apixaban, or edoxaban were enrolled, and a single steady-state trough concentration was measured. FXaI concentrations were compared with the expected range reported in clinical trials to define high or low drug levels. The primary outcome was major bleeding, and the secondary outcome was ischemic stroke or transient ischemic attack (IS/TIA). From 2016 to 2023, 1,037 patients aged from 30 to 105 years were enrolled (average, 75.4 ± 10.0 years; 33.8% were aged ≥ 80 years). During a median follow-up of 2.35 years, 48 major bleeding events and 32 IS/TIA events were observed. Although drug concentrations were similar between the two age groups, those aged ≥ 80 years with high FXaI levels experienced a greater increase in major bleeding risk compared to those aged < 80 years with high levels (aHR 6.47 [2.07, 20.28] vs. 3.45 [1.15, 10.30]). Additionally, patients aged ≥ 80 years without elevated FXaI levels also had a higher risk of major bleeding compared to those aged < 80 years without elevated levels (aHR 2.39 [1.20, 4.76]). While low FXaI concentrations were associated with IS/TIA, the risk was not significantly different across age groups. In conclusion, despite similar FXaI concentrations, patients aged ≥ 80 years have a higher baseline risk of major bleeding and experience a greater increase in bleeding risk at high drug levels compared to those aged < 80 years.
© 2025 The Author(s). Clinical Pharmacology & Therapeutics published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures

Similar articles
-
Incidence and Predictors of Clinical Outcomes in Real-Life Patients With Atrial Fibrillation Treated With Oral Factor Xa Inhibitors: The Follow-Up Results of the ANATOLIA-AF Study.Clin Cardiol. 2025 Jan;48(1):e70088. doi: 10.1002/clc.70088. Clin Cardiol. 2025. PMID: 39871620 Free PMC article.
-
Non-Vitamin K Antagonist Oral Anticoagulants and Factors Influencing the Ischemic and Bleeding Risk in Elderly Patients With Atrial Fibrillation: A Review of Current Evidence.J Cardiovasc Pharmacol. 2020 Oct 14;77(1):11-21. doi: 10.1097/FJC.0000000000000927. J Cardiovasc Pharmacol. 2020. PMID: 33060545 Free PMC article. Review.
-
Microdosed Cocktail of Three Oral Factor Xa Inhibitors to Evaluate Drug-Drug Interactions with Potential Perpetrator Drugs.Clin Pharmacokinet. 2019 Sep;58(9):1155-1163. doi: 10.1007/s40262-019-00749-1. Clin Pharmacokinet. 2019. PMID: 30828771 Clinical Trial.
-
Effectiveness and Safety of Apixaban, Dabigatran, and Rivaroxaban Versus Warfarin in Patients With Nonvalvular Atrial Fibrillation and Previous Stroke or Transient Ischemic Attack.Stroke. 2017 Aug;48(8):2142-2149. doi: 10.1161/STROKEAHA.117.017474. Epub 2017 Jun 27. Stroke. 2017. PMID: 28655814
-
Comparative effectiveness of rivaroxaban in the treatment of nonvalvular atrial fibrillation.J Comp Eff Res. 2017 Sep;6(6):549-560. doi: 10.2217/cer-2017-0025. Epub 2017 Jul 24. J Comp Eff Res. 2017. PMID: 28737102 Free PMC article. Review.
References
-
- Sun, J. , Qiao, Y. , Zhao, M. , Magnussen, C.G. & Xi, B. Global, regional, and national burden of cardiovascular diseases in youths and young adults aged 15‐39 years in 204 countries/territories, 1990‐2019: a systematic analysis of global burden of disease study 2019. BMC Med. 21, 222 (2023). - PMC - PubMed
-
- Patel, M.R. et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 365, 883–891 (2011). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
