

General Anesthesia Versus Conscious Sedation in Thrombectomy Patients With Low NIHSS Anterior Circulation Stroke
- PMID: 40130311
- PMCID: PMC12036785
- DOI: 10.1161/STROKEAHA.124.049358
General Anesthesia Versus Conscious Sedation in Thrombectomy Patients With Low NIHSS Anterior Circulation Stroke
Abstract
Background: The optimal anesthetic approach for patients with acute ischemic stroke with large vessel occlusion but low National Institutes of Health Stroke Scale receiving mechanical thrombectomy remains unclear. We aimed to evaluate the association of anesthetic strategies with procedural and clinical outcomes, hypothesizing that conscious sedation/local anesthesia (CS/LA) may offer a more favorable risk-benefit ratio than general anesthesia (GA).
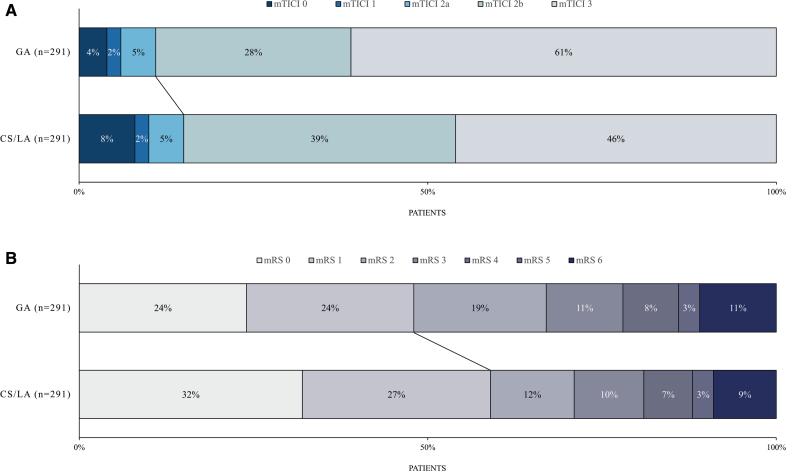
Methods: Multicenter cohort study screening all thrombectomy patients prospectively enrolled in GSR-ET (German Stroke Registry-Endovascular Treatment) across 25 centers between 2015 and 2021. Patients with an admission National Institutes of Health Stroke Scale score of <6 and large vessel occlusion in the anterior circulation underwent 1:1 propensity score matching by their anesthetic strategy during mechanical thrombectomy (CS/LA versus GA). Outcome measures were an excellent functional outcome (modified Rankin Scale score of 0-1 at 90 days) and successful recanalization (modified Thrombolysis in Cerebral Infarction score of 2b-3).
Results: Of 13 082 thrombectomy cases, 814 had a National Institutes of Health Stroke Scale <6, of whom 36% received CS/LA and 64% received GA. Before matching, CS/LA patients were less often male (46% versus 54%; P=0.043), had lower National Institutes of Health Stroke Scale scores at admission (median, 3 versus 4; P=0.002), and the M1 segment of the middle cerebral artery was more often occluded (51% versus 39%; P<0.001). After matching, 582 patients were included, and baseline and imaging characteristics were balanced between CS/LA and GA. CS/LA and GA patients achieved similar rates of successful recanalization (85% versus 89%; P=0.14). However, complete recanalization (modified Thrombolysis in Cerebral Infarction score of 3) was less often observed in CS/LA patients (45% versus 61%; P<0.001; adjusted odds ratio, 0.44 [95% CI, 0.30-0.65]; P<0.001). CS/LA patients achieved more often excellent functional outcomes (59% versus 48%; P=0.005; adjusted odds ratio, 1.99 [95% CI, 1.34-2.95]; P=0.001).
Conclusions: In thrombectomy patients with minor stroke, the rate of successful recanalization was comparable between CS/LA and GA. However, our results suggest a more favorable risk-benefit ratio of CS/LA, with an increased rate of excellent functional outcomes.
Keywords: angiography; cohort studies; registries; stroke; thrombectomy.
Conflict of interest statement
Dr Flottmann reported receiving personal fees from Eppdata GmbH outside the submitted work. Dr Kniep reported an ownership stake in Eppdata GmbH and compensation from Eppdata GmbH for consultant services outside the submitted work. Dr Faizy reported grants from the German Research Foundation/Deutsche Forschungsgesellschaft (DFG; project number: 411621970) and personal fees from Eppdata GmbH outside the submitted work. Dr Broocks reported grants from the American Society of Neuroradiology and receiving compensation as a speaker from Balt and personal fees from Eppdata GmbH outside the submitted work. Dr Meyer reported receiving compensation as a speaker from Balt and personal fees from Eppdata GmbH outside the submitted work. Dr Thaler reported receiving personal fees from Eppdata GmbH outside the submitted work. Dr Thomalla reported grants from FP7 Health and grants from AstraZeneca. In addition, he reported receiving personal fees from Acandis, Alexion, Amarin, Bayer, Boehringer Ingelheim, Bristol Myers Squibb/Pfizer, Daiichi Sankyo, Portola, and Stryker outside the submitted work. Dr Fiehler reported stock holdings in Tegus Medical; compensation from Tonbridge for consultant services; stock holdings in Vastrax; compensation from Roche for consultant services; compensation from TG Medical for consultant services; and compensation from Penumbra Inc for consultant services. In addition, he reported an ownership stake in Eppdata GmbH and grants and personal fees from Acandis, Cerenovus, MicroVention, Medtronic, Stryker, and Phenox and grants from Route 92 outside the submitted work. The other authors report no conflicts.
Figures
References
-
- Seners P, Cereda CW. Thrombectomy in stroke with a large vessel occlusion and mild symptoms: “striving to better, oft we mar what’s well?”. Stroke. 2023;54:2276–2278. doi: 10.1161/STROKEAHA.123.044205 - PubMed
-
- Nogueira RG. Endovascular therapy for low NIHSS ischemic strokes. clinicaltrials.gov; 2022. [cited June 8, 2023]. https://clinicaltrials.gov/ct2/show/NCT04167527
-
- University Hospital, Montpellier. Evaluation of acute mechanical revascularization in large vessel occlusion stroke with minor symptoms (NIHSS<6) in patients last seen well < 24 hours. clinicaltrials.gov; 2022. [cited June 8, 2023]. https://clinicaltrials.gov/ct2/show/NCT03796468
-
- Schönenberger S, Hendén PL, Simonsen CZ, Uhlmann L, Klose C, Pfaff JAR, Yoo AJ, Sørensen LH, Ringleb PA, Wick W, et al. . Association of general anesthesia vs procedural sedation with functional outcome among patients with acute ischemic stroke undergoing thrombectomy: a systematic review and meta-analysis. JAMA. 2019;322:1283–1293. doi: 10.1001/jama.2019.11455 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
