

Intravenous immunoglobulin as first-line acute treatment in adults with autoimmune encephalitis caused by antibodies to NMDAR, LGI1 and CASPR2
- PMID: 40131535
- PMCID: PMC11937155
- DOI: 10.1007/s00415-025-13032-0
Intravenous immunoglobulin as first-line acute treatment in adults with autoimmune encephalitis caused by antibodies to NMDAR, LGI1 and CASPR2
Abstract
Background and objectives: Corticosteroids or plasma exchange are recommended for acute treatment of autoimmune encephalitis (AE). Intravenous immunoglobulins (IVIG) are suggested as an additional treatment option but data on treatment effect is scarce. The objective of the present study was to investigate the impact of the first-line treatment on the three most common forms of AE, in particular, to evaluate the effect of IVIG therapy in these diseases.
Methods: A total of 1274 patients from the German Network for Autoimmune Encephalitis Research (GENERATE) were analyzed, and 388 patients were included in the study because they had either anti-NMDAR, anti-LGI1 or anti-CASPR2 antibodies and firs-line immunotherapy (ivMP monotherapy, ivMP + IVIG, ivMP + PE or ivMP + IVIG + PE) or no immunotherapy at all. For the statistical analyses, patients were stratified according to antibody type, distinguishing between anti-NMDAR (IgG1) and anti-LGI1 as well as anti-CASPR2 (predominantly IgG4). The primary endpoint was the clinical outcome at discharge, which was assessed using the modified Rankin Scale (mRS). The mRS scores were then compared between the different treatment groups over time, and the factors influencing the reduction in mRS at discharge were analyzed. Furthermore, a specific investigation was conducted to determine the differences in outcomes between patients treated with ivMP + IVIG and ivMP + PE, each split by antibody subtype.
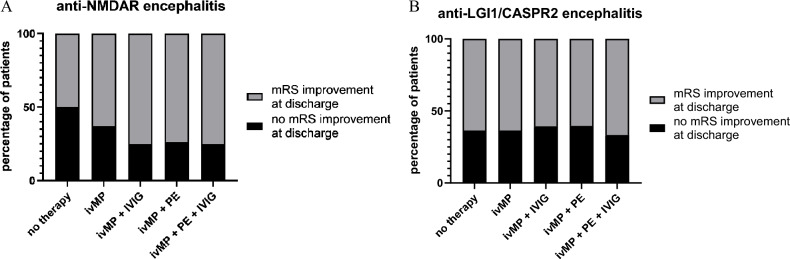
Results: In all treatment groups analyzed, significant improvements were observed at the time of discharge and after 12 months compared to disease onset, regardless of the type of first-line treatment. In untreated patients a significant improvement was not observed. The choice of IVIG or PE as an additional treatment to ivMP for anti-NMDAR encephalitis did not affect the primary outcome. In anti-LGI1 or anti-CASPR2 encephalitis, no influence on the primary outcome was observed when IVIG or PE was administered in addition to ivMP, too. However, a direct comparison of the individual antibody subgroups' mRS reductions, depending on the treatment approach (ivMP + IVIG vs. ivMP + PE), revealed that a more significant mRS reduction was observed with ivMP + PE in anti-NMDAR encephalitis.
Discussion: The retrospective data give evidence that there is no difference in outcome for the use of ivMP + PE over ivMP + IVIG or vice versa in the treatment of encephalitis caused by antibodies against NMDAR, LGI1 or CASPR2. Furthermore, the specific method of plasma exchange, whether plasmapheresis or immunoadsorption, did not affect the mRS at discharge.
Keywords: Autoimmune encephalitis; CASPR2; IVIG; Immunotherapy; LGI-1; NMDA.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors have no conflicts of interest to declare. MS is employee of Novartis. Ethics approval and consent to participate: All aspects of the study have been conducted in accordance with the declaration of Helsinki. Ethical review and approval were not required for the study on human participants according to local legislation and institutional requirements. The patient himself or a legal guardian of the patient gave written informed consent to participate in this study.
Figures





References
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
