

Evaluation of postural therapy using lateral position according to fetal back orientation on breech presentation and breech recurrence (BRLT study): An open-label randomized controlled trial
- PMID: 40132016
- PMCID: PMC11936219
- DOI: 10.1371/journal.pmed.1004555
Evaluation of postural therapy using lateral position according to fetal back orientation on breech presentation and breech recurrence (BRLT study): An open-label randomized controlled trial
Abstract
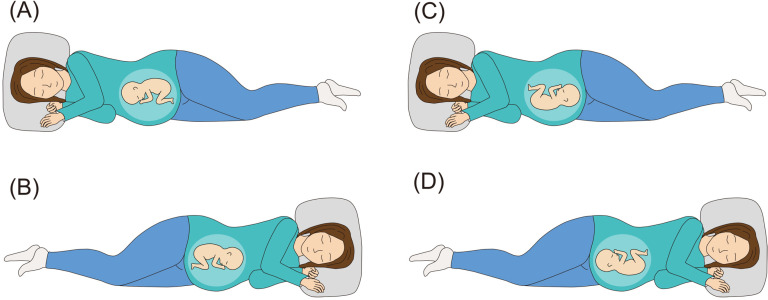
Background: In Japan, the lateral position method is known as a postural therapy for breech presentation wherein the mother lies down in lateral position according to the orientation of the fetal back. Few studies have formally tested lateral position management for breech presentation, and no method exists to prevent breech recurrence after cephalic version. We hypothesized that postural management comprising a combination of opposite-side lateral position for breech presentation and same-side lateral position after cephalic version demonstrates a clinically relevant effect size on breech presentation.
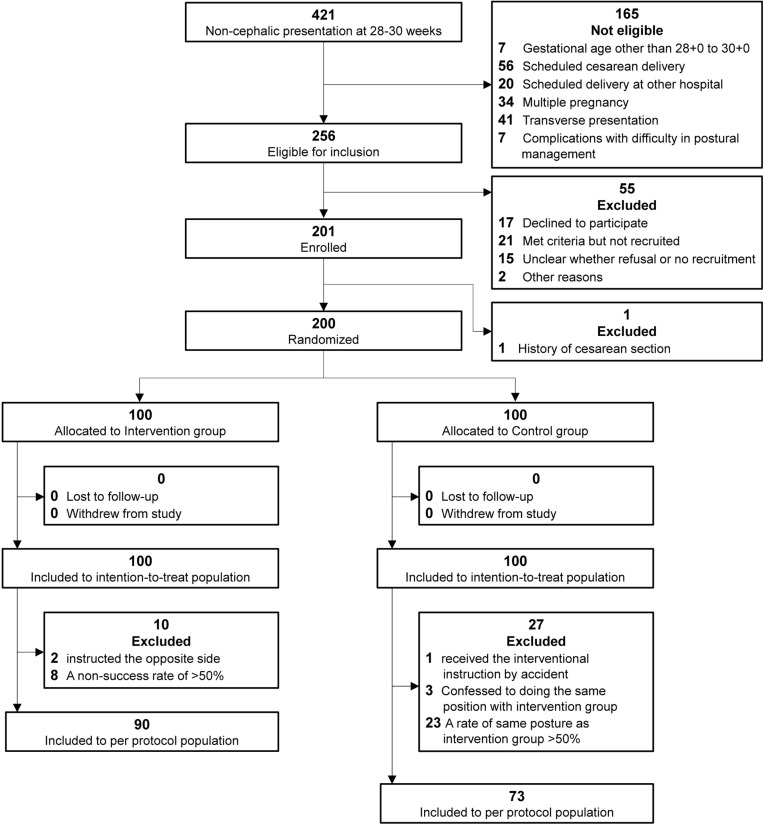
Methods and findings: We conducted a stratified, open-label randomized controlled trial at an academic hospital in Kawasaki, Japan. A total of 200 women diagnosed with breech presentation between 28 + 0 and 30 + 0 gestational weeks were randomized to postural management (n = 100) or control (no intervention, n = 100) group. The intervention was instruction every 2 weeks on lying in the lateral position on the opposite-side of fetal back for breech presentation and on the same-side of fetal back for head-first presentation. The primary outcome was the rate of fetuses in breech presentation at 37 weeks of gestation, and the secondary outcomes were cesarean delivery, cesarean delivery for breech presentation, head presentation 2, 4, and 6 weeks later, breech presentation recurrence, and adverse events. Breech presentation rate at 37 gestational weeks was 11% in the intervention group, using the combination of the opposite-side and same-side lateral positions, compared with 19% in the control group. However, we found no statistical significance in the intention-to-treat analysis (11% [11/100] versus 19% [19/100]; relative risk, 0.58 [95% CI, 0.29 to 1.15]; p = 0.11). In the control group, 23 participants (23%) unknowingly took the same posture as the intervention group, and the prespecified per-protocol analysis excluding crossover found the same direction of effect but with statistical significance. In the intention-to-treat analysis, the intervention group had a higher cephalic version rate 2 weeks after the instruction (69% [69/100] versus 54% [54/100]; relative risk, 0.67 [95% CI, 0.47 to 0.96]; p = 0.029), and lower breech presentation recurrence rates (2% [2/91] versus 10% [9/88]; relative risk, 0.22 [95% CI, 0.048 to 0.97]; p = 0.031) than the control group. Regarding adverse events in the intervention group, three participants experienced discomfort and one participant complained of pain in the lateral abdomen; these symptoms resolved spontaneously.
Conclusions: For breech presentation at the beginning of the third trimester, providing postural therapy instruction on opposite-side lateral positioning and same-side lateral positioning was associated with 8% reduction of breech fetuses at 37 gestational weeks compared with the control group, but this primary endpoint did not reach statistical significance. Regarding the secondary endpoints, the intervention group showed a significantly higher rate of cephalic version after 2 weeks and lower rate of breech recurrence. The direction of the effect of postural therapy based on fetal back position on breech presentation was promising, and further research to validate this approach, with consideration for unplanned participant crossover, may be warranted.
Trial registration: UMIN Clinical Trials Registry (UMIN000043613, https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000049800).
Copyright: © 2025 Shinmura et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Hannah ME, Hannah WJ, Hewson SA, Hodnett ED, Saigal S, Willan AR. Planned caesarean section versus planned vaginal birth for breech presentation at term: a randomised multicentre trial. Term Breech Trial Collaborative Group. Lancet. 2000;356(9239):1375–83. doi: 10.1016/s0140-6736(00)02840-3 - DOI - PubMed
-
- Sagawa K, Suzuki S, Takeda S, Kinoshita K. Trends in mode of breech delivery in Japan. Hypertens Res Preg. 2021;9:26–9.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
