

Assessing differential application of thromboprophylaxis regimes related to risk of pulmonary embolism and mortality in COVID-19 patients through instrumental variable analysis
- PMID: 40133355
- PMCID: PMC11937556
- DOI: 10.1038/s41598-024-77858-w
Assessing differential application of thromboprophylaxis regimes related to risk of pulmonary embolism and mortality in COVID-19 patients through instrumental variable analysis
Abstract
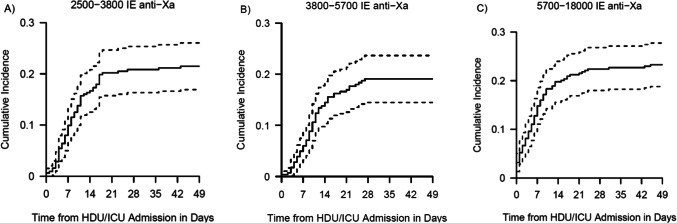
Thrombotic complications are common in Coronavirus disease 2019 (COVID-19) patients, with pulmonary embolism (PE) being the most frequent. Randomised trials have provided inconclusive results on the optimal dosage of thromboprophylaxis in critically ill COVID-19 patients. We utilized data from the multicentre CAPACITY-COVID patient registry to assess the effect of differential application of Low Molecular Weight Heparin (LMWH) dose protocols on PE and in-hospital mortality risk in critically ill COVID-19 patients. An instrumental variable analysis was performed to estimate the intention-to-treat effect, utilizing differences in thromboprophylaxis prescribing behaviour between hospitals. We included 939 patients with PCR confirmed SARS-CoV-2 infection from 34 hospitals. Two-hundred-and-one patients (21%) developed a PE. The adjusted cause-specific HR of PE was 0.92 (95% CI: 0.73-1.16) per doubling of LMWH dose. The adjusted cause-specific HR for in-hospital mortality was 0.82 (95% CI: 0.65-1.02) per doubling of LMWH dose. This dose-response relationship was shown to be non-linear. To conclude, this study did not find evidence for an effect of LMWH dose on the risk of PE, but suggested a non-linear decreased risk of in-hospital mortality for higher doses of LMWH. However, uncertainty remains, and the dose-response relationship between LMWH dose and in-hospital mortality needs further investigation in well-designed studies.
Keywords: COVID-19; Dose–response relationship; Drug; Heparin; Hospital mortality; Low-molecular-weight; Pulmonary embolism.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: Frederikus A. Klok reports grants or contracts from Bayer, BMS, BSCI, MSD, Leo Pharma, Actelion, Pharm-X, The Netherlands Organisation for Health Research and Development, The Dutch Thrombosis Association, The Dutch Heart Foundation and the Horizon Europe Program, all unrelated to this work and paid to his institution. Karina Meijer has received consulting fees from Uniqure and speaker fees from Alexion, Bayer and CSL Behring paid to her institution. Roger E. G. Schutgens has received unrestricted grants paid to the department for research outside this work from Bayer, CSL Behring, Novartis, NovoNordisk, Octapharma, Roche and Sobi. Alexander P. J. Vlaar has received consulting fees from InflaRx paid to his institution. Folkert W. Asselbergs has received payments from UCL Hospitals NIHR Biomedical Research Centre paid to himself. Marieke J. H. A. Kruip has received unrestricted grants paid to the department for research outside this CSL Behring. The other authors have no relevant financial or non-financial interests to disclose.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
