

"Pharmacological management of acute agitation in psychiatric patients: an umbrella review"
- PMID: 40133850
- PMCID: PMC11934566
- DOI: 10.1186/s12888-024-06426-3
"Pharmacological management of acute agitation in psychiatric patients: an umbrella review"
Abstract
Background: The main characteristics present in patients with psychomotor agitation include restlessness, excessive motor activity, irritability, and heightened responsiveness to internal and external stimuli. This umbrella review evaluates the efficacy and safety of pharmacological interventions for patients with psychiatric disorders presenting psychomotor agitation, aged 18 years or older. A comprehensive literature search was conducted to identify umbrella reviews that met our study's inclusion criteria. However, no reviews were found that specifically investigated the efficacy and safety of pharmacological interventions for agitated psychiatric patients presenting with both behavioral and psychological symptoms, such as emotional lability, decreased attention span, and cognitive and behavioral alterations. The primary objective is to assess the effectiveness of pharmacological interventions in controlling patients within a short time frame, measured in hours rather than days. The focus was placed on studies addressing treatment in emergency settings, whether in general hospitals or psychiatric facilities, with an emphasis on managing acute psychomotor agitation rather than long-term maintenance treatment.
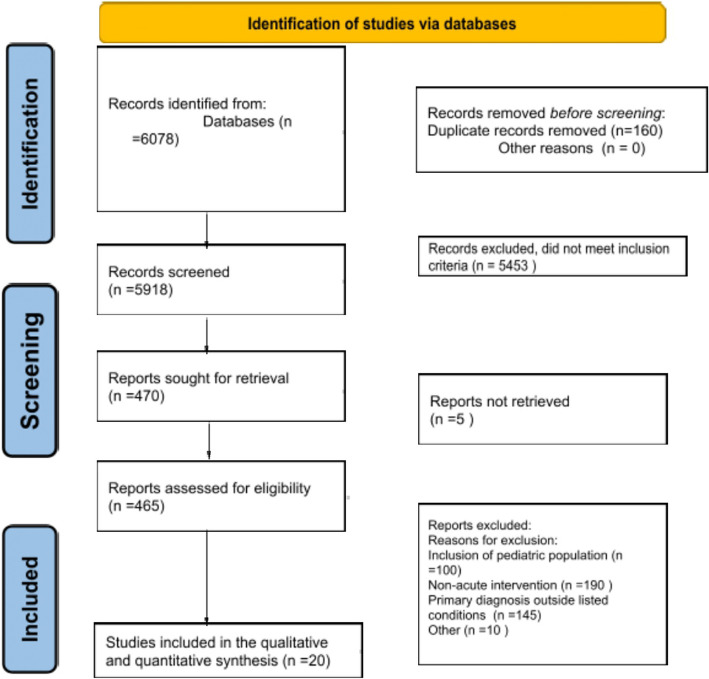
Method: A comprehensive literature search for meta-analyses and systematic reviews assessing the efficacy and safety of pharmacological treatment for psychomotor agitation in psychiatric inpatients and emergency department patients was conducted across various databases such as PubMed, Scopus, EMBASE, Web of Science and COCHRANE Central database. Included reviews comprised those that incorporated randomized controlled trials (RCTs) or non-randomized controlled trials (NRCTs) comparing the efficacy and safety of pharmacological interventions for agitated psychiatric patients (with both psychological and behavioral symptoms).
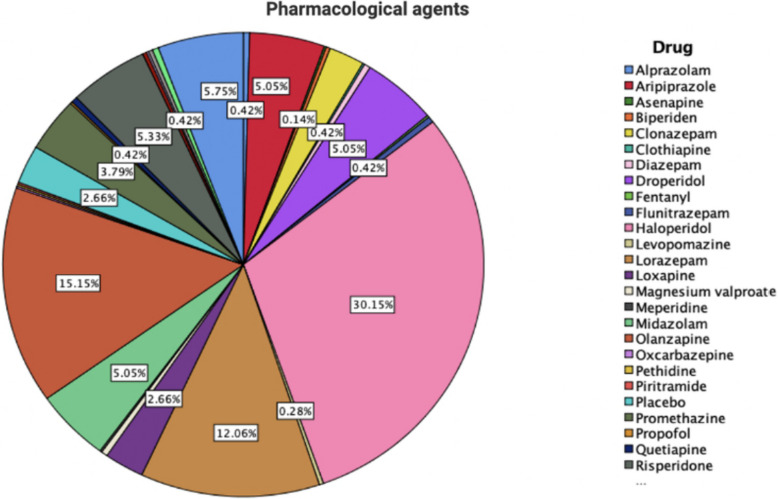
Results: Loxapine (10 mg) demonstrated superior efficacy over 5 mg in reducing agitation within 120 min, with inhaled formulations providing rapid relief in patients with acute psychosis. Aripiprazole was effective and caused less sedation compared to Olanzapine, although Haloperidol required fewer additional doses but was less effective at 60 min. Ziprasidone, administered intramuscularly, offered a faster onset and was better tolerated than Haloperidol. Lorazepam proved effective with fewer side effects than antipsychotics and showed enhanced efficacy when combined with them. Midazolam provided rapid sedation but posed risks of severe side effects, especially in older adults. Droperidol was as effective as Olanzapine but provided faster sedation. Combination therapy, such as Haloperidol with Promethazine, effectively reduced aggression with a lower incidence of adverse effects.
Conclusion: This umbrella review offers a comprehensive overview of the pharmacological management of psychomotor agitation in patients with psychiatric disorders. Among the most frequently used medications in the reviewed studies were haloperidol, olanzapine, and lorazepam. The findings underscore the importance of tailored treatment approaches and the need for further research to refine the management of psychomotor agitation in psychiatric settings.
Keywords: Antipsychotics; Benzodiazepines; Bipolar disorders; Psychotic disorders.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: The authors consent for publication in order of the policies of BMC Psychiatry. Competing interests: The authors declare no competing interests.
Figures
References
-
- Pacciardi B, Mauri M, Cargioli C, Belli S, Cotugno B, Di Paolo L, et al. Issues in the management of acute agitation: how much current guidelines consider safety? Front Psychiatry. 2013;4. Available from: http://journal.frontiersin.org/article/10.3389/fpsyt.2013.00026/abstract. Cited 2023 Nov 15. - DOI - PMC - PubMed
-
- Nordstrom K, Allen MH. Managing the acutely agitated and psychotic patient. CNS Spectr. 2007;12(S17):5–11. - PubMed
-
- Soyka M. Aggression in schizophrenia: assessment and prevalence. Br J Psychiatry. 2002;180(3):278–9. - PubMed
-
- Allen MH, Currier GW. Use of restraints and pharmacotherapy in academic psychiatric emergency services. Gen Hosp Psychiatry. 2004;26(1):42–9. - PubMed
-
- Citrome L. New treatments for agitation. Psychiatr Q. 2004;75(3):197–213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
