

Computerized tomography angiography in diagnosing an obtuse marginal branch perforation after pericardiocentesis: a case report
- PMID: 40134987
- PMCID: PMC11932988
- DOI: 10.3389/fcvm.2025.1535797
Computerized tomography angiography in diagnosing an obtuse marginal branch perforation after pericardiocentesis: a case report
Abstract
Background: Pericardiocentesis is both therapeutic and diagnostic invasive procedure, guided by echocardiography and/or angiography. It can be done using subcostal or apical approach. One of the major complications of pericardiocentesis is coronary artery laceration with an incidence of less than 1%. Diagnosis of such lacerations is often made by invasive coronary angiography or urgent thoracotomy. Computed tomography angiography is used to determine the extent of bleeding and hemopericardium, but its potential for detailed evaluation of bleeding site is somewhat underestimated.
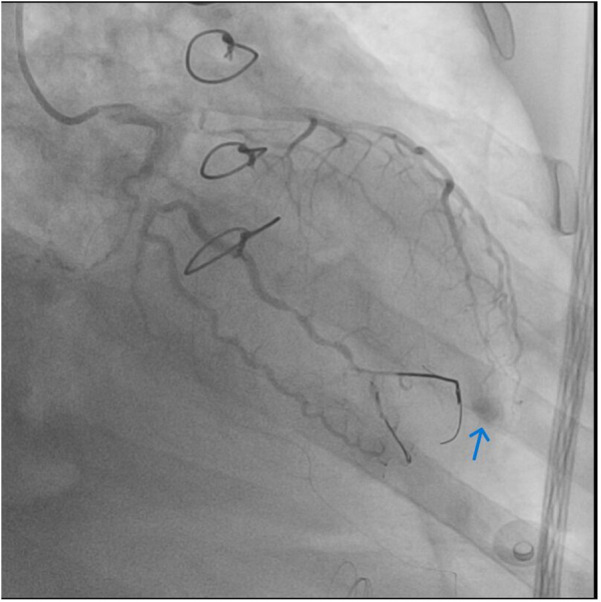
Case presentation: We present a rare case of distal obtuse marginal (OM) artery perforation resulting from apical pericardiocentesis that was diagnosed with CT angiography (CTA) further treated with coronary guidewire particle embolization. A 49-year-old male patient who had undergone ascending aorta and aortic arch reconstruction after an aortic dissection Type A was evaluated with echocardiography before being discharged from our hospital. A loculated pericardial effusion was identified, necessitating pericardiocentesis. The clinical course was further complicated by hemopericardium due to coronary laceration. The hemorrhage was managed with coronary guidewire segment embolization which led to immediate improvement in hemodynamic status. The patient was discharged seven days after intervention.
Conclusion: Coronary artery perforation is a rare, albeit life-threatening complication of pericardiocentesis that requires urgent surgical or percutaneous intervention. CTA can provide important diagnostic information on perforation location and help in deciding whether embolization or open-heart surgery is needed to address ongoing bleeding.
Keywords: aortic dissection; computed tomography angiography; coronary laceration; obtuse marginal; pericardiocentesis.
© 2025 Ostojic, Antonic and Ilic.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Ingraham A, Sperry J. Operative management of cardiac injuries: diagnosis, technique, and postoperative complications. Curr Trauma Rep. (2015) 1:225–31. 10.1007/s40719-015-0032-9 - DOI
Publication types
LinkOut - more resources
Full Text Sources