

Deep Learning for Ultrasonographic Assessment of Temporomandibular Joint Morphology
- PMID: 40137567
- PMCID: PMC11946603
- DOI: 10.3390/tomography11030027
Deep Learning for Ultrasonographic Assessment of Temporomandibular Joint Morphology
Abstract
Background: Temporomandibular joint (TMJ) disorders are a significant cause of orofacial pain. Artificial intelligence (AI) has been successfully applied to other imaging modalities but remains underexplored in ultrasonographic evaluations of TMJ.
Objective: This study aimed to develop and validate an AI-driven method for the automatic and reproducible measurement of TMJ space width from ultrasonographic images.
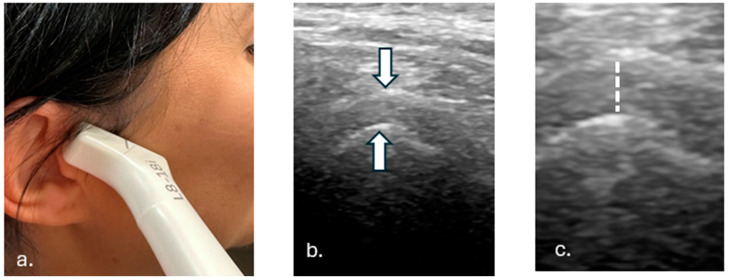
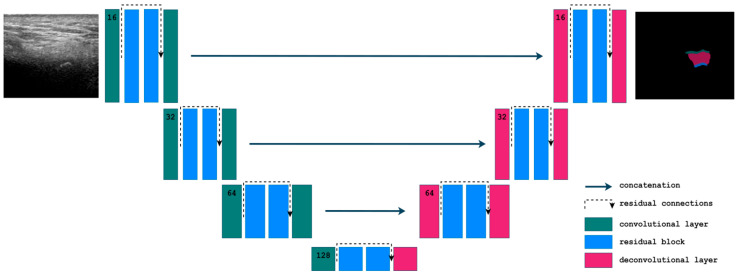
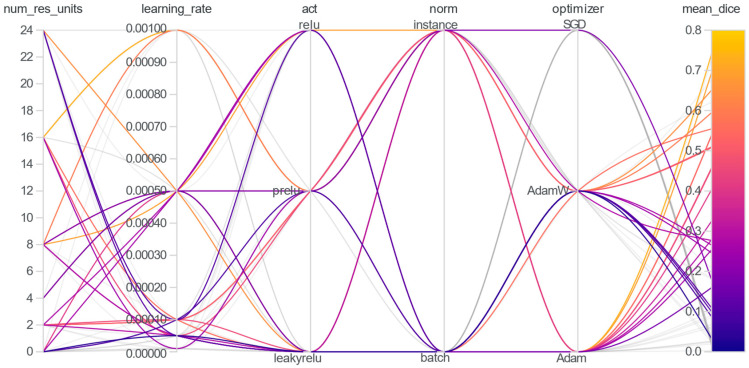
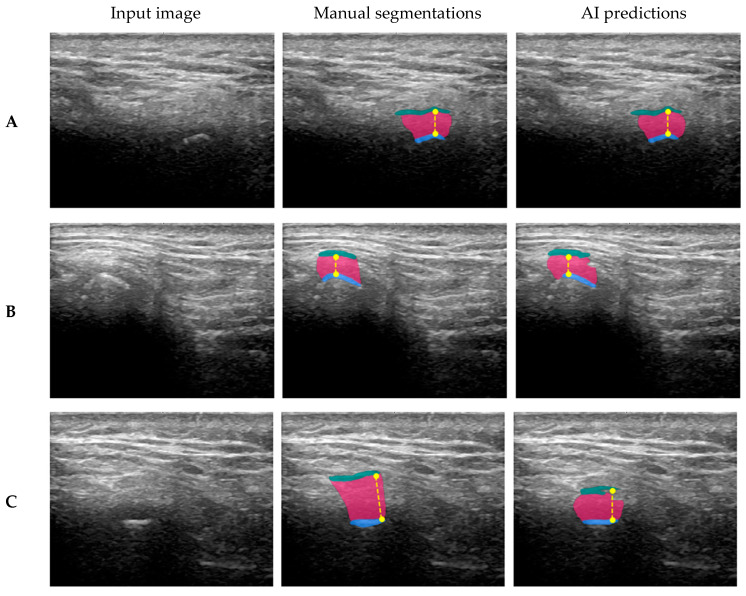
Methods: A total of 142 TMJ ultrasonographic images were segmented into three anatomical components: the mandibular condyle, joint space, and glenoid fossa. State-of-the-art architectures were tested, and the best-performing 2D Residual U-Net was trained and validated against expert annotations. The algorithm for joint space width measurement based on TMJ segmentation was proposed, calculating the vertical distance between the superior-most point of the mandibular condyle and its corresponding point on the glenoid fossa.
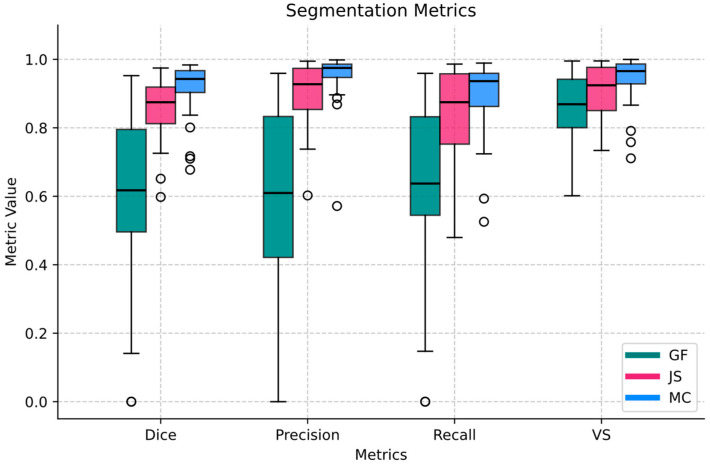
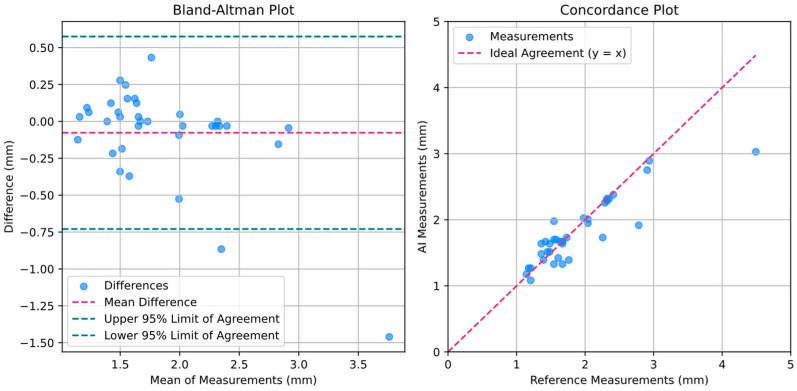
Results: The segmentation model achieved high performance for the mandibular condyle (Dice: 0.91 ± 0.08) and joint space (Dice: 0.86 ± 0.09), with notably lower performance for the glenoid fossa (Dice: 0.60 ± 0.24), highlighting variability due to its complex geometry. The TMJ space width measurement algorithm demonstrated minimal bias, with a mean difference of 0.08 mm and a mean absolute error of 0.18 mm compared to reference measurements.
Conclusions: The model exhibited potential as a reliable tool for clinical use, demonstrating accuracy in TMJ ultrasonographic analysis. This study underscores the ability of AI-driven segmentation and measurement algorithms to bridge existing gaps in ultrasonographic imaging and lays the foundation for broader clinical applications.
Keywords: artificial intelligence; deep learning; temporomandibular joints; ultrasonography.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Deep learning for automated segmentation of the temporomandibular joint.J Dent. 2023 May;132:104475. doi: 10.1016/j.jdent.2023.104475. Epub 2023 Mar 2. J Dent. 2023. PMID: 36870441
-
Temporomandibular joint segmentation in MRI images using deep learning.J Dent. 2022 Dec;127:104345. doi: 10.1016/j.jdent.2022.104345. Epub 2022 Nov 8. J Dent. 2022. PMID: 36368120
-
Automated pediatric TMJ articular disk identification and displacement classification in MRI with machine learning.J Dent. 2025 Apr;155:105622. doi: 10.1016/j.jdent.2025.105622. Epub 2025 Feb 13. J Dent. 2025. PMID: 39952550
-
Ultrasonography of the temporomandibular joint: a literature review.Int J Oral Maxillofac Surg. 2009 Dec;38(12):1229-36. doi: 10.1016/j.ijom.2009.07.014. Epub 2009 Aug 22. Int J Oral Maxillofac Surg. 2009. PMID: 19700262 Review.
-
Temporomandibular joint assessment in MRI images using artificial intelligence tools: where are we now? A systematic review.Dentomaxillofac Radiol. 2025 Jan 1;54(1):1-11. doi: 10.1093/dmfr/twae055. Dentomaxillofac Radiol. 2025. PMID: 39563454 Free PMC article.
Cited by
-
A Deep Learning Approach for Mandibular Condyle Segmentation on Ultrasonography.J Imaging Inform Med. 2025 May 6. doi: 10.1007/s10278-025-01527-1. Online ahead of print. J Imaging Inform Med. 2025. PMID: 40329156
-
AI in Medical Imaging and Image Processing.J Clin Med. 2025 Jun 11;14(12):4153. doi: 10.3390/jcm14124153. J Clin Med. 2025. PMID: 40565899 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
