

SAMHD1 dysfunction impairs DNA damage response and increases sensitivity to PARP inhibition in chronic lymphocytic leukemia
- PMID: 40140468
- PMCID: PMC11947222
- DOI: 10.1038/s41598-025-93629-7
SAMHD1 dysfunction impairs DNA damage response and increases sensitivity to PARP inhibition in chronic lymphocytic leukemia
Abstract
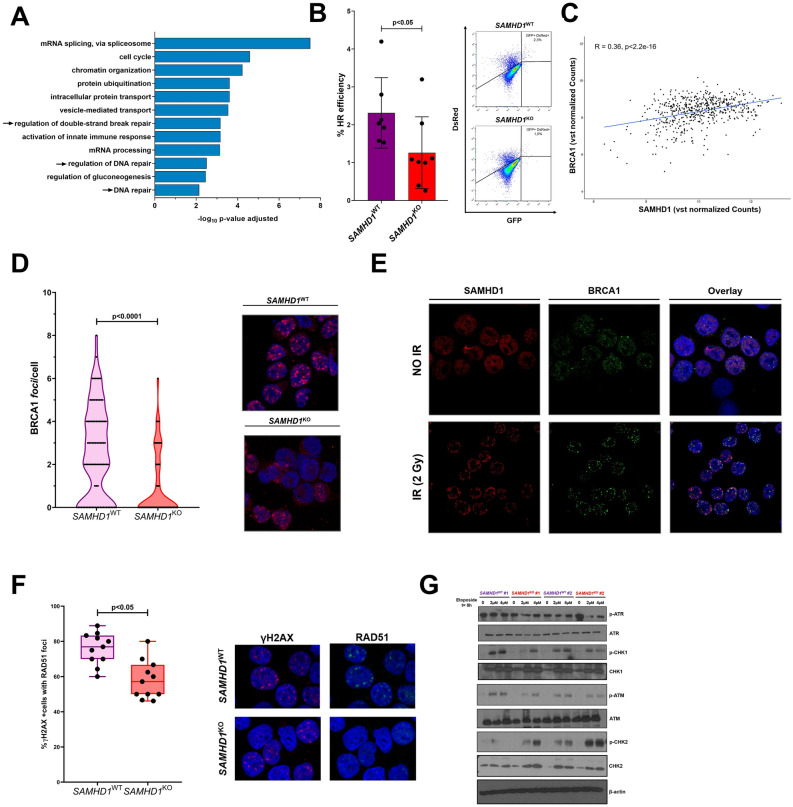
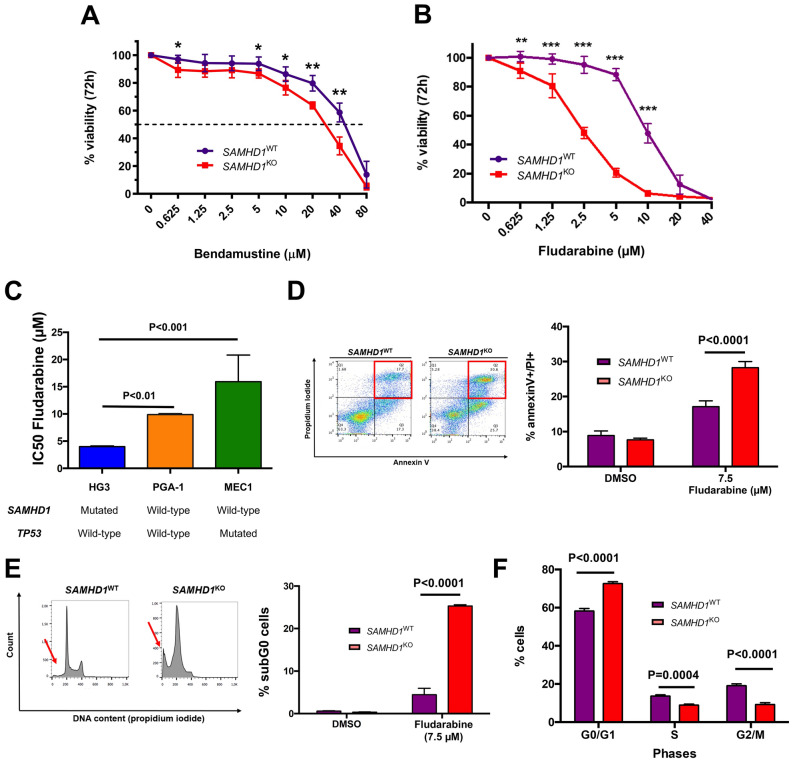
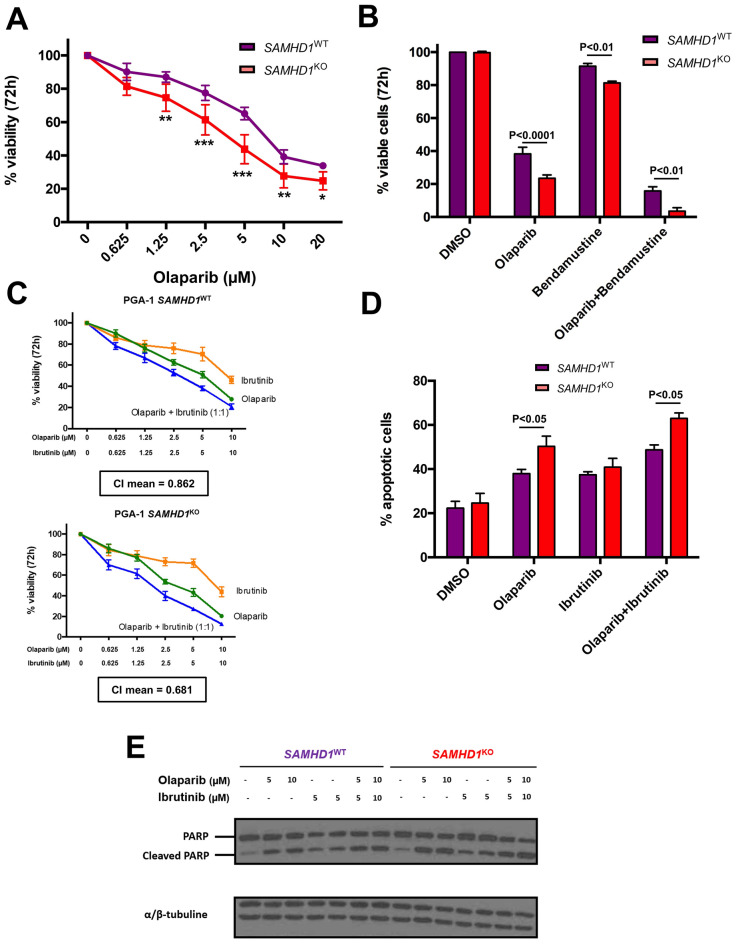
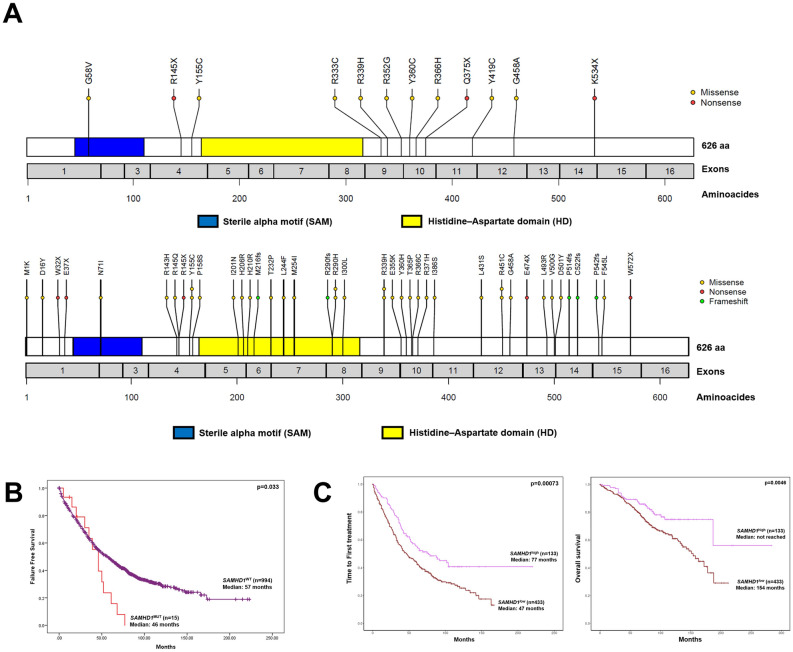
Chronic lymphocytic leukemia (CLL) is a clinically and genetically heterogenous disease. Recent next-generation sequencing (NGS) studies have uncovered numerous low-frequency mutated genes in CLL patients, with SAMHD1 emerging as a candidate driver gene. However, the biological and clinical implications of SAMHD1 mutations remain unclear. Using CRISPR/Cas9, we generated CLL models to investigate the impact of SAMHD1 deficiency on pathogenesis and explore therapeutic strategies. Moreover, we performed NGS in treatment-naïve CLL patients to characterize SAMHD1 mutations and employed RNA-sequencing to evaluate their clinical significance. Our study shows that SAMHD1 inactivation impairs the DNA damage response by reducing homologous recombination efficiency through BRCA1 and RAD51 dysregulation. Importantly, SAMHD1 colocalizes with BRCA1 at DNA damage sites in CLL cells. This research also identifies that SAMHD1-mutated cells are more sensitive to PARP inhibition. Clinically, SAMHD1 dysfunction negatively impacts clinical outcome of CLL cases: SAMHD1 mutations reduce failure-free survival (median 46 vs 57 months, p = 0.033), while low SAMHD1 expression associates with shorter time to first treatment (median 47 vs 77 months; p = 0.00073). Overall, this study elucidates that SAMHD1 dysfunction compromises DNA damage response mechanisms, potentially contributing to unfavorable clinical outcomes in CLL, and proposes PARP-inhibitors as a potential therapeutic approach for SAMHD1-mutated CLL cells.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethics declarations: This study was approved by the ethics committee of Hospital Universitario de Salamanca and written informed consent was obtained from all participants before they entered the study in accordance to the declaration of Helsinki.
Figures
Similar articles
-
CRISPR/Cas9-generated models uncover therapeutic vulnerabilities of del(11q) CLL cells to dual BCR and PARP inhibition.Leukemia. 2020 Jun;34(6):1599-1612. doi: 10.1038/s41375-020-0714-3. Epub 2020 Jan 23. Leukemia. 2020. PMID: 31974435 Free PMC article.
-
SAMHD1 is mutated recurrently in chronic lymphocytic leukemia and is involved in response to DNA damage.Blood. 2014 Feb 13;123(7):1021-31. doi: 10.1182/blood-2013-04-490847. Epub 2013 Dec 12. Blood. 2014. PMID: 24335234 Free PMC article.
-
Poly(ADP-ribose) polymerase inhibitor CEP-8983 synergizes with bendamustine in chronic lymphocytic leukemia cells in vitro.Leuk Res. 2014 Mar;38(3):411-7. doi: 10.1016/j.leukres.2013.12.019. Epub 2013 Dec 30. Leuk Res. 2014. PMID: 24439051 Free PMC article.
-
Use of poly ADP-ribose polymerase [PARP] inhibitors in cancer cells bearing DDR defects: the rationale for their inclusion in the clinic.J Exp Clin Cancer Res. 2016 Nov 24;35(1):179. doi: 10.1186/s13046-016-0456-2. J Exp Clin Cancer Res. 2016. PMID: 27884198 Free PMC article. Review.
-
Next-generation sequencing in chronic lymphocytic leukemia.Semin Hematol. 2013 Oct;50(4):286-95. doi: 10.1053/j.seminhematol.2013.09.005. Semin Hematol. 2013. PMID: 24246696 Review.
References
-
- Zenz, T., Mertens, D., Küppers, R., Döhner, H. & Stilgenbauer, S. From pathogenesis to treatment of chronic lymphocytic leukaemia. Nat. Rev. Cancer10(1), 37–50 (2010). - PubMed
-
- Puente, X. S. et al. Non-coding recurrent mutations in chronic lymphocytic leukaemia. Nature526(7574), 519–524 (2015). - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
