

Vaginal host immune-microbiome-metabolite interactions associated with spontaneous preterm birth in a predominantly white cohort
- PMID: 40140683
- PMCID: PMC11947164
- DOI: 10.1038/s41522-025-00671-4
Vaginal host immune-microbiome-metabolite interactions associated with spontaneous preterm birth in a predominantly white cohort
Abstract
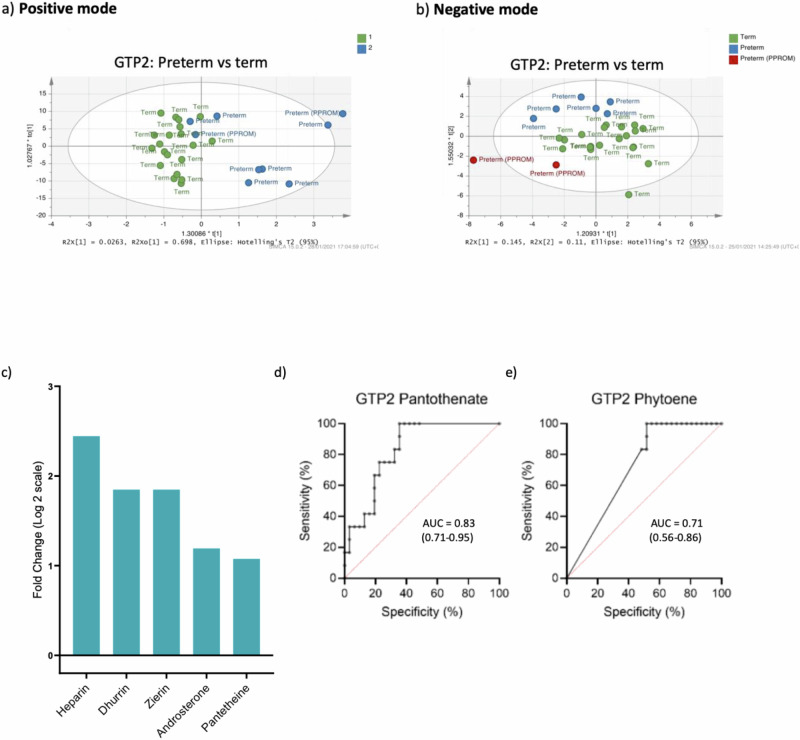
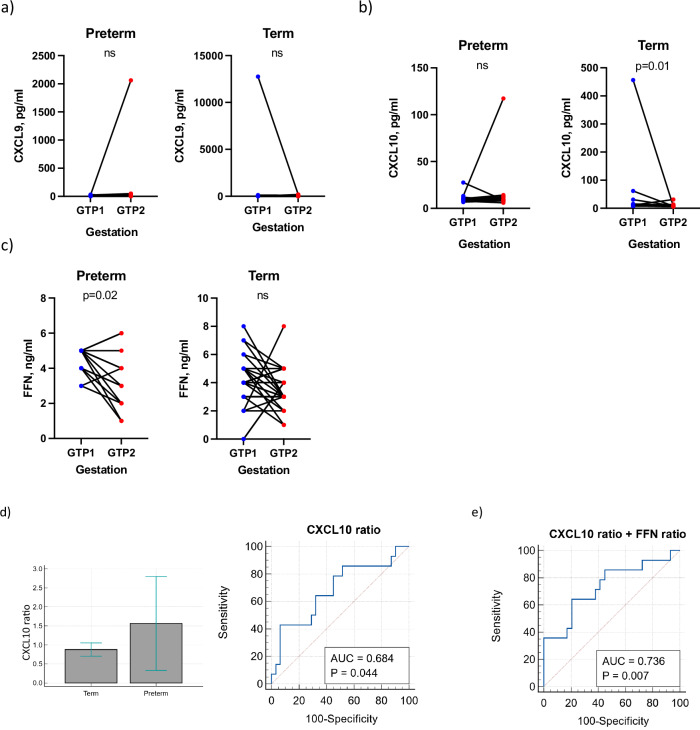
In order to improve spontaneous preterm birth (sPTB) risk stratification in a predominantly white cohort of non-labouring pregnant women, we analysed their vaginal microbiota, metabolite, cytokine and foetal fibronectin (FFN) concentrations at two gestational time points (GTPs): GTP1 (20+0-22+6 weeks, preterm = 17; term = 32); and GTP2 (26+0-28+6 weeks, preterm = 14; term = 31). At GTP1, the preterm-delivered women showed abundant G. vaginalis (AUC = 0.77) over L. crispatus and L. iners, and upregulation of 10 metabolites. At GTP2, the same women had more lactobacilli- and mixed anaerobes-dominated microbiota, upregulation of five metabolites, and decreased TNFR1, distinguishing them from their term counterparts (AUC = 0.88). From GTP1 to GTP2, sPTB was associated with increased microbiota α-diversity, and upregulation of pantothenate and urate. CXCL10 declined in the term-delivered women by ~3-fold, but increased in the preterm-delivered women (AUC = 0.68), enhanced by FFN (AUC = 0.74). Characterising the complex dynamic interactions between cervicovaginal microbial metabolites and host immune responses could enhance sPTB risk stratification.
© 2025. Crown.
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures











References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
