

Comparing Italian versus European strategies and technologies for respiratory care in NICU: results of a survey of the Union of European Neonatal and Perinatal Societies (UENPS) and the Italian Society of Neonatology (SIN)
- PMID: 40140879
- PMCID: PMC11948922
- DOI: 10.1186/s13052-025-01936-6
Comparing Italian versus European strategies and technologies for respiratory care in NICU: results of a survey of the Union of European Neonatal and Perinatal Societies (UENPS) and the Italian Society of Neonatology (SIN)
Abstract
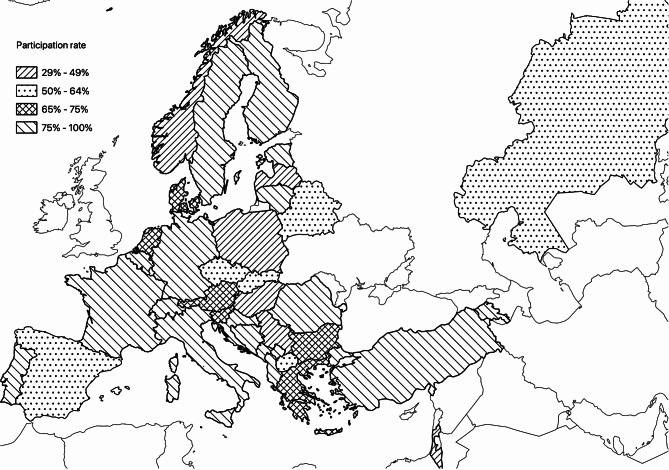
Background: Our survey aimed to compare information on respiratory care in Neonatal Intensive Care Units (NICUs) in Italy and in the European and Mediterranean region.
Methods: Cross-sectional electronic survey. An 89-item questionnaire focusing on the current modes, devices, and strategies employed in neonatal units in the domain of respiratory care was sent to directors/heads of 528 NICUs.
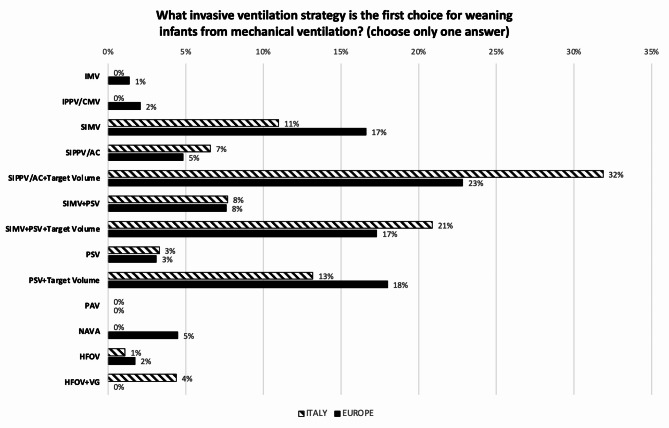
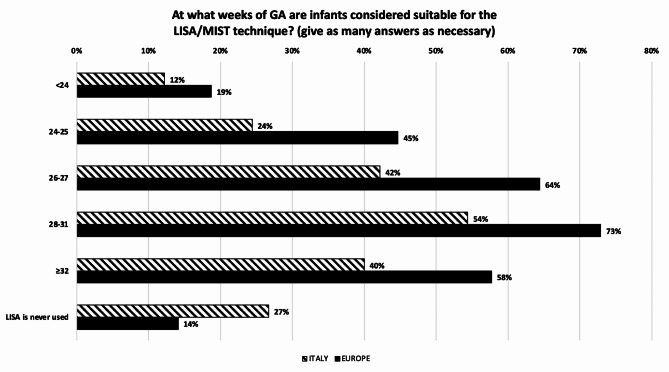
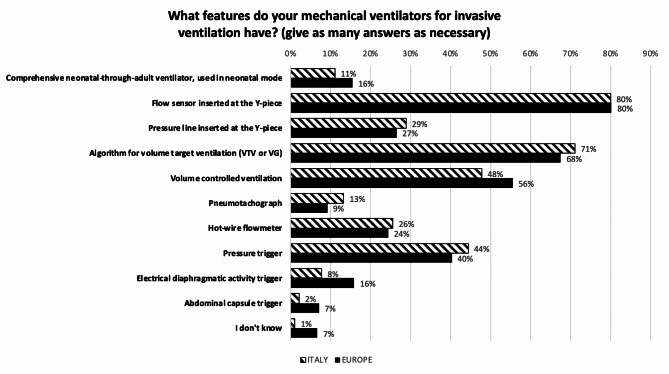
Results: The response rate was 75% (397/528 units). The median number of NICU beds and the admission rate per unit/year of preterm infants < 1500 g was significantly lower in Italy compared with Europe (p < 0.001). In most Italian Delivery Rooms (DR) full resuscitation is given from 22 to 23 weeks gestational age, while 21.0% of the European units initiate from 24 weeks. Initial FiO2 is set as per American Academy of Pediatrics guidelines in 81.1% of Italian units compared to 30.9% of the European ones (p < 0.001). DR surfactant is less often given through Less-Invasive-Surfactant-Administration (LISA) in Italy (53.4% vs. 76.2% of units, p < 0.03). Volume-targeted, synchronized intermittent positive-pressure ventilation (IPPV) is the preferred invasive mechanical ventilation (MV) mode to treat acute RDS across the surveyed units, however 22.9% % of Italian centers vs. 6.8% of the European ones use HFOV as first choice (p < 0.001). During HFOV, 78% of Italian NICUs set mean airway pressure (MAP) following a lung recruitment procedure compared to 41% of the centers in Europe (p < 0.001). In the NICUs, most of the non-invasive (NIV) modes used are nasal CPAP and nasal IPPV. For infants on NIV, LISA strategy is used in 25.6% of Italian vs. 60.0% of European units (p < 0.001). 70% of surveyed units use a brand caffeine. Inhaled steroids are used in 42.3% of Italian vs. 65.4% of European NICUs (p < 0.001).
Conclusions: respiratory support strategies among the surveyed Italian and European NICUs are quite dissimilar in some areas, particularly where high-quality evidence is lacking. We believe that hese data will allow stakeholders to make comparisons and to identify opportunities for improvement.
Keywords: Caffeine; Delivery room; Mechanical ventilation; Preterm infants; RDS; Steroids; Surfactant; Survey.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was submitted to the Ethics Committee of the Azienda Ospedale Università di Padova, which reviewed it and awarded an exemption letter (protocol n. 396n/AO/23, 20 July 2023), as not meeting criteria for human subject research. The authors confirm that all methods were performed in accordance with the ethical standards as laid down in the Declaration of Helsinki and its later amendments or comparable ethical standards. Consent for publication: Not applicable. Competing interest: The authors declare that they have no competing interest regarding the publication of this article.
Figures




References
-
- Belteki G, Morley CJ. High-frequency oscillatory ventilation with volume guarantee: a single-centre experience. Arch Dis Child Fetal Neonatal Ed. 2019;104(4):F384–9. 10.1136/archdischild-2018-315490 - PubMed
-
- Tana M, Paladini A, Tirone C, Aurilia C, Lio A, Bottoni A et al. Effects of high-frequency oscillatory ventilation with volume guarantee during surfactant treatment in extremely low gestational age newborns with respiratory distress syndrome: an observational study. Front Pediatr. 2022;9:804807. 10.3389/fped.2021.804807. eCollection 2021. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
