

Altered Pharmacokinetics of Ropivacaine in Patients Undergoing Laparoscopic Major Hepatectomy
- PMID: 40143048
- PMCID: PMC11944703
- DOI: 10.3390/pharmaceutics17030386
Altered Pharmacokinetics of Ropivacaine in Patients Undergoing Laparoscopic Major Hepatectomy
Abstract
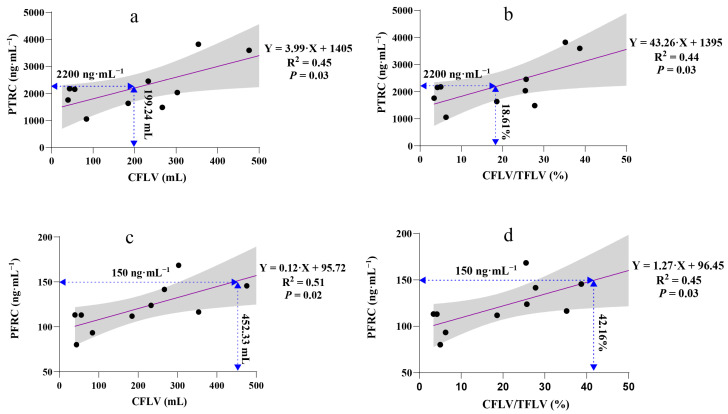
Background/Objectives: Ropivacaine is primarily metabolized by the liver. High doses of ropivacaine, combined with altered pharmacokinetics due to hepatectomy, raise concerns about potential drug toxicity. We investigated the impact of LMH (laparoscopic major hepatectomy) on the pharmacokinetics of high-dose ropivacaine. Methods: Ten patients undergoing LMH received a BD-TAP (bilateral dual transversus abdominis plane) block with a high dose of ropivacaine (3 mg·kg-1 in 60 mL). Plasma concentrations of total and free ropivacaine and AAG (alpha-1 acid glycoprotein) levels were measured. Liver volumes were calculated using three-dimensional liver reconstruction technology. Results: The peak total ropivacaine concentration occurred 45 min after the block, reaching 2031.5 (876.0) ng·mL-1, with a tendency to exceed the toxicity threshold in patients with a CFLV (cut functional liver volume) exceeding 199.24 mL or a CFLV/TFLV (total functional liver volume) ratio surpassing 18.61%. The peak free ropivacaine concentration, 111.5 (31.3) ng·mL-1, was observed 90 min after the block, potentially exceeding the toxicity threshold when CFLV exceeded 452.33 mL or the CFLV/TFLV ratio was greater than 42.16%. Plasma AAG levels increased approximately 1.5 times within 24 h, from 1519.7 (422.6) μg·mL-1 preoperatively to 2253.6 (460.4) μg·mL-1 postoperatively, effectively reducing the toxicity risk associated with free ropivacaine. Conclusions: Preoperative administration of high-dose ropivacaine can be safely utilized in patients undergoing major hepatectomy. The increased plasma AAG concentration due to surgical stress reduces free ropivacaine levels, enhancing patient tolerance to the drug. The CFLV and CFLV/TFLV ratio may be supplementary indicators for predicting ropivacaine toxicity.
Keywords: alpha-1 acid glycoprotein; bilateral dual transversus abdominis plane block; laparoscopic major hepatectomy; local anesthetic toxicity; ropivacaine.
Conflict of interest statement
The authors declare no conflicts of interest in this work.
Figures


References
-
- Leone S., Di Cianni S., Casati A., Fanelli G. Pharmacology, toxicology, and clinical use of new long acting local anesthetics, ropivacaine and levobupivacaine. Acta Biomed. 2008;79:92–105. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
