

Trends in stroke incidence, death, and disability outcomes in a multi-ethnic population: Auckland regional community stroke studies (1981-2022)
- PMID: 40143891
- PMCID: PMC11938151
- DOI: 10.1016/j.lanwpc.2025.101508
Trends in stroke incidence, death, and disability outcomes in a multi-ethnic population: Auckland regional community stroke studies (1981-2022)
Abstract
Background: Reliable data on trends of stroke incidence and outcomes over time are necessary for assessing the effectiveness of public health and clinical strategies, and for allocating healthcare resources. We assessed the levels and trends in incidence, mortality, early case fatality and disability for stroke in a defined, ethnically mixed population over 40 years.
Methods: To analyse data from five population-based stroke incidence studies in adult residents (age ≥15 years) of the Greater Auckland Region of New Zealand (NZ) (1.35 million) over 12-month calendar periods for 1981-1982, 1991-1992, 2002-2003, 2011-2012, and 2021-2022. Fatal and non-fatal, hospitalised and non-hospitalised stroke events (first-ever and recurrent) were identified through multiple overlapping sources using clinical World Health Organization (WHO) diagnostic criteria and neuroimaging to define three major pathological types of stroke: ischaemic stroke (IS), primary intracerebral haemorrhage (PICH), subarachnoid haemorrhage (SAH), and stroke of undetermined type (SUT). Crude and age-standardised annual incidence, mortality, 28-day case fatality and disability level, and 40-year trends were calculated by age, sex, and ethnicity assuming a Poisson distribution. For comparison of our findings, we carried out a pooled analysis of methodologically comparable population-based stroke epidemiology estimates in high-income countries over the last two decades.
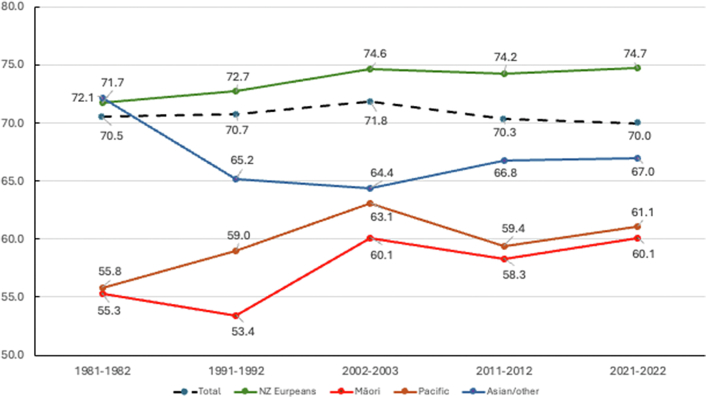
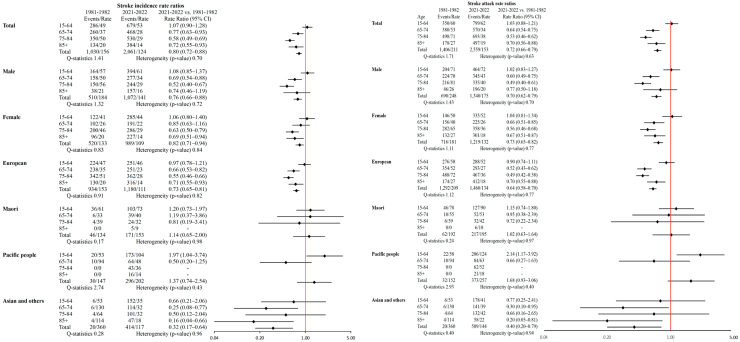
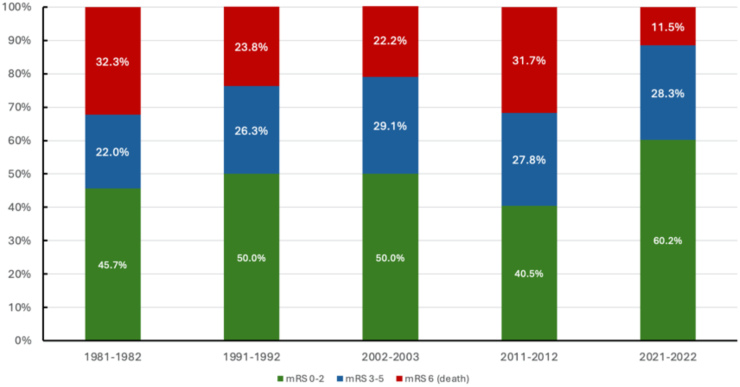
Findings: Overall, there were 7462 first-ever strokes (9917 events) over the 40-year period (4,682,012 person-years). From 1981-1982 to 2021-2022, age-standardised stroke incidence rates decreased from 156/100,000 (95% confidence interval [CI] 143; 170) to 124/100,000 (119; 130) and mortality rates from 98/100,000 (88; 110) to 28/100,000 (26; 31) in nearly all age, sex, and ethnic groups. Moreover, from 2002-2003 to 2021-2022, there was an increase in stroke incidence of 1.28% per year (95% CI 0.38-2.17) in people aged 15-54 years, with the mean age of people with stroke decreasing from 73.0 (SD ± 13.8) in 2002-2003 to 71.6 (SD ± 14.9) in 2011-2012 and 70.7 (SD ± 15.2) years in 2021-2022 (p for trend <0.0001). The risk of stroke in Māori and Pacific people in 2021-2022 was almost 1.5 and 2.0 times greater than that in NZ Europeans. Ethnic disparities in the risk of stroke and age of stroke onset remained stable over the study period. From 1981-1982 to 2021-2022, 28-day stroke case fatality declined from 33.1% to 12.1% (p < 0.0001). There was a trend towards reducing 28-day case-fatality (from 31.6% [95% CI 27.6; 35.7] in 1981-1982 to 11.4% [10.0; 12.7] in 2021-2022) and an increasing proportion of stroke survivors with good functional outcome at discharge/28-days post-stroke (increased from 45.7% (95% CI 41.3; 50.0) in 1981-1982 to 60.2% (58.1; 62.3) in 2021-2022).
Interpretation: Stroke incidence, 1-year mortality and 28-day case-fatality and disability have decreased in Auckland, NZ over the last 4 decades. However, over the last decade (2011-2022) there was a stagnation in the decline in the age-standardised stroke incidence rates. The absolute numbers of people with strokes, and those who have died or remained disabled from stroke, have significantly increased from 1981 to 2022. Ethnic disparities in the risk and burden of stroke persist. Effective prevention strategies for stroke must remain a high priority.
Funding: Health Research Council of New Zealand.
Keywords: Disability; Incidence; Mortality; Outcomes; Stroke; Trends.
© 2025 The Author(s).
Conflict of interest statement
VLF declares that he is a CEO of the New Zealand Stroke Education (charitable) Trust that provides online free of charge stroke self-management rehabilitation videos. CSA received research grants, consulting fees and honoraria from AstraZeneca, works as President-elect of World Stroke Organisation and Editor-in-Chief of Cerebrovascular Diseases; PAB is President Australia and New Zealand Association of Neurologists; AR received consulting fees from Australian Health Department, works in Stroke Foundation NZ, Australian and NZ Stroke Organisation, and World Stroke Organisation. Other authors declare no conflict of interest.
Figures
References
-
- Sun J., Qiao Y., Zhao M., Magnussen C.G., Xi B. Global, regional, and national burden of cardiovascular diseases in youths and young adults aged 15-39 years in 204 countries/territories, 1990-2019: a systematic analysis of Global Burden of Disease Study 2019. BMC Med. 2023;21:222. doi: 10.1186/s12916-023-02925-4. - DOI - PMC - PubMed
