

Minimally Invasive Myomectomy with Temporary Bilateral Uterine Artery Blockage at Anterior Cul-de-Sac
- PMID: 40144384
- PMCID: PMC11935644
- DOI: 10.4293/JSLS.2024.00078
Minimally Invasive Myomectomy with Temporary Bilateral Uterine Artery Blockage at Anterior Cul-de-Sac
Abstract
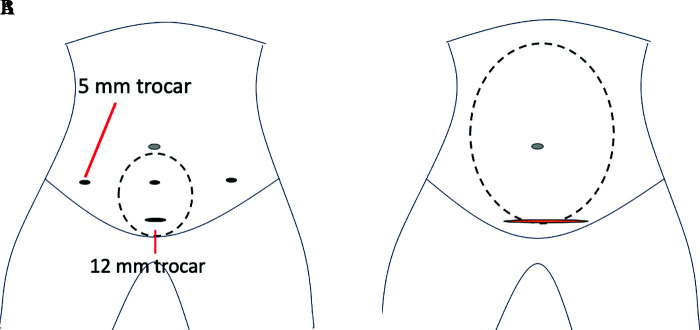
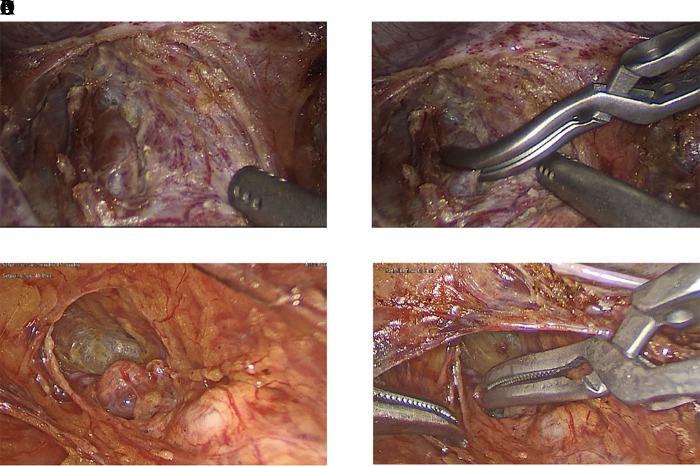
Background and objectives: Minimizing intraoperative bleeding is pivotal in myomectomy, and blockage of uterine arteries has been reported as an effective approach. We developed a novel technique to temporary occlude bilateral uterine arteries at the anterior cul-de-sac in minimally invasive myomectomy (MIS), including minilaparotomy, laparoscopic-assisted myomectomy, and laparoscopic myomectomy. This study aims to evaluate the intraoperative and postoperative outcomes of this technique in complicated myomectomy cases.
Methods: Twenty-seven patients underwent minimally invasive myomectomy by single minimally invasive surgeon using bilateral uterine arteries blockage. To match the complexity of myomectomy, 66 open cases performed by generalists were used for control.
Results: There were no significant differences in fibroid size, number, or weight between MIS and open myomectomy groups. For intraoperative outcomes, the MIS group showed longer operative time (271.3 ± 72.9 vs 179.9 ± 78.8 minutes, P < .05), but fewer cases of intraoperative blood transfusion (3% vs 17%, P < .05) and fewer intraoperative complications (0% vs 3%, P < .005). For postoperative outcomes, the MIS group demonstrated shorter hospital stay (70% vs 29% for 0-1 day; 11% vs 42% for 2 days; 19% vs 29% for 3 or more days, P < .05) and fewer postoperative complications (3% vs 9%, P < .05).
Conclusion: Temporary blockage bilateral uterine arteries enable the safe performance of complicated myomectomy via minimally invasive surgery.
Keywords: Bulldog; Minimally invasive surgery; Myomectomy; Uterine artery.
© 2025 by SLS, Society of Laparoscopic & Robotic Surgeons.
Conflict of interest statement
Conflict of interests: none.
Figures
Similar articles
-
Laparoscopic Myomectomy with Temporary Bilateral Uterine Artery and Utero-Ovarian Vessels Occlusion Compared with Traditional Surgery for Uterine Fibroids: Blood Loss and Recurrence.Gynecol Obstet Invest. 2019;84(6):548-554. doi: 10.1159/000499494. Epub 2019 Apr 9. Gynecol Obstet Invest. 2019. PMID: 30965324
-
Predictors of Overnight Admission After Laparoscopic Myomectomy in a High-Volume Minimally Invasive Gynecologic Surgery Setting.J Minim Invasive Gynecol. 2020 Jan;27(1):195-199. doi: 10.1016/j.jmig.2019.03.022. Epub 2019 Mar 29. J Minim Invasive Gynecol. 2020. PMID: 30936030
-
Laparoscopic Myomectomy with Temporary Bilateral Uterine Artery Occlusion Compared with Traditional Surgery for Uterine Myomas: Blood Loss and Recurrence.J Minim Invasive Gynecol. 2018 Mar-Apr;25(3):434-439. doi: 10.1016/j.jmig.2017.06.032. Epub 2017 Sep 21. J Minim Invasive Gynecol. 2018. PMID: 28943191 Clinical Trial.
-
Surgical outcomes after uterine artery occlusion at the time of myomectomy: systematic review and meta-analysis.Fertil Steril. 2019 Apr;111(4):816-827.e4. doi: 10.1016/j.fertnstert.2018.12.011. Epub 2019 Jan 17. Fertil Steril. 2019. PMID: 30661604
-
In-bag manual versus uncontained power morcellation for laparoscopic myomectomy.Cochrane Database Syst Rev. 2020 May 6;5(5):CD013352. doi: 10.1002/14651858.CD013352.pub2. Cochrane Database Syst Rev. 2020. PMID: 32374421 Free PMC article.
Cited by
-
Advances and Challenges in Minimally Invasive Myomectomy: A Narrative Review.J Clin Med. 2025 Jun 17;14(12):4313. doi: 10.3390/jcm14124313. J Clin Med. 2025. PMID: 40566056 Free PMC article. Review.
References
-
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. 2003;188(1):100–107. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical