

Long-Acting Growth Hormone for Pediatric Growth Hormone Deficiency
- PMID: 40144813
- PMCID: PMC11938432
- DOI: 10.1210/jendso/bvaf040
Long-Acting Growth Hormone for Pediatric Growth Hormone Deficiency
Abstract
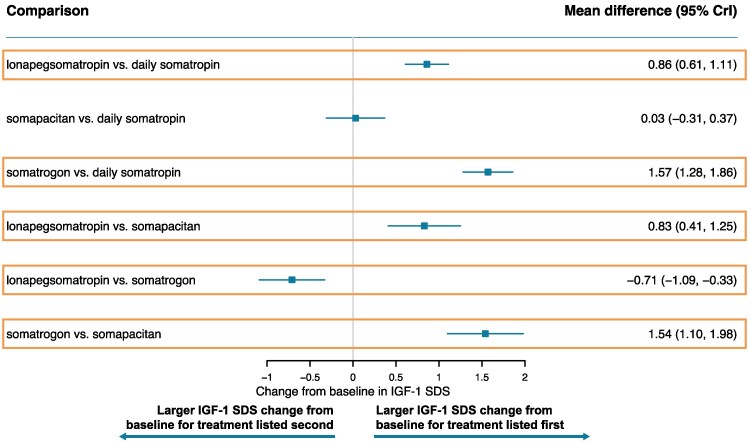
Long-acting growth hormone (LAGH) has the potential to improve adherence and outcomes over daily somatropin in growth hormone deficiency (GHD). Whereas daily somatropin products are molecularly identical, LAGHs are molecularly distinct; additional moieties or mechanisms that prolong LAGH action confer unique pharmacodynamic/pharmacokinetic properties that could affect efficacy and safety. Only one LAGH available in the United States and Europe (lonapegsomatropin) delivers unmodified somatropin. With no head-to-head clinical trials of LAGHs available, this systematic literature review and network meta-analysis were conducted to compare the relative efficacy and safety of LAGHs in pediatric GHD. Five trials were eligible for inclusion in a Bayesian network meta-analysis; 3 contributed to the base case network, including 3 LAGHs (lonapegsomatropin, somapacitan, and somatrogon) and daily somatropin. Treatment with lonapegsomatropin was associated with statistically significantly higher annualized height velocity and change from baseline in height SD score (SDS) at week 52 compared to daily somatropin and somapacitan; no other significant differences in these outcomes were found. The change from baseline in average insulin-like growth factor-1 (IGF-1) SDS at week 52 was significantly higher for somatrogon vs all comparators and for lonapegsomatropin vs daily somatropin and somapacitan; average IGF-1 SDS was within normal range in all trials. No significant differences were seen in progression in bone age-to-chronological age ratio or serious adverse events (SAEs). Sensitivity analyses were consistent with the base case. In this network meta-analysis, lonapegsomatropin was the only LAGH associated with better growth outcomes. No significant differences were detected regarding SAEs; other safety outcomes could not be analyzed.
Keywords: literature review; long-acting growth hormone; meta-analysis; pediatric growth hormone deficiency.
© The Author(s) 2025. Published by Oxford University Press on behalf of the Endocrine Society.
Figures






References
-
- Brinkman JE, Tariq MA, Leavitt L, Sharma S. Physiology, Growth Hormone. StatPearls Publishing LLC; 2024. StatPearls. StatPearls Publishing. Copyright © 2024.
-
- Maruff P, Falleti M. Cognitive function in growth hormone deficiency and growth hormone replacement. Horm Res. 2005;64 Suppl 3:100‐108. - PubMed
-
- Betts JG. Bone tissue and skeletal system; the endocrine system. In: Anatomy and Physiology. Rice University; 2022:661‐709.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous