

Computed tomography identifies sex-specific differences in surgical chronic thromboembolic pulmonary hypertension
- PMID: 40145035
- PMCID: PMC11935516
- DOI: 10.1016/j.jhlto.2024.100130
Computed tomography identifies sex-specific differences in surgical chronic thromboembolic pulmonary hypertension
Abstract
Background: Registry data suggest women are less likely than men to undergo pulmonary thromboendarterectomy for chronic thromboembolic pulmonary hypertension despite a similar proportion of proximal vs distal disease. We hypothesized that sex-specific differences could be elicited with a computed tomography pulmonary angiography analysis beyond proximal vs distal.
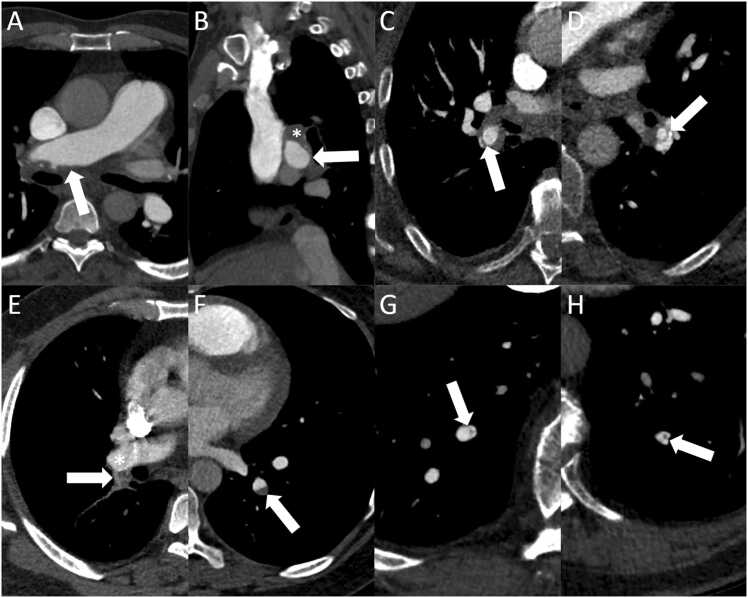
Methods: Preoperative computed tomography pulmonary angiography of patients who underwent pulmonary thromboendarterectomy for chronic thromboembolic pulmonary hypertension from January 2017 to September 2021 was analyzed. The pulmonary vascular tree was divided into 32 named vessels with chronic thromboembolism presence and lesion type recorded for each vessel. If no lesion was identified in a segmental vessel, subsegmental disease was recorded when present.
Results: One hundred forty-four patients (mean age 57 ± 15 years, 78 women) were included. There were no sex differences in baseline hemodynamics. Men had more vessels involved than women (mean 20.3 vs 17.1, p = 0.004) and had fewer disease-free pulmonary segments (mean 4.9 ± 4.3 vs 7.6 ± 5.5, p = 0.001). Men had a greater number of webs, eccentric thickening, and occlusions. The distribution of lesion type did not significantly differ between sexes at the main or lobar level but men had significantly more lesions in the segmental vasculature while women had a higher proportion of subsegmental lesions (p < 0.001).
Conclusions: Sex-specific differences in chronic thromboembolic pulmonary hypertension are demonstrated on computed tomography pulmonary angiography in overall distribution and lesion type at the segmental and subsegmental level with women having fewer and more distal lesions despite similar hemodynamics.
Keywords: chronic pulmonary embolism; chronic thromboembolic pulmonary hypertension; computed tomography; pulmonary angiography; pulmonary thromboendarterectomy.
© 2024 International Society for Heart and Lung Transplantation.
Conflict of interest statement
Micheal McInnis reports financial support was provided by Joint Department of Medical Imaging Academic Incentive Fund. Marc de Perrot reports a relationship with AstraZeneca Pharmaceuticals LP that includes consulting or advisory, Bristol Myers Squibb Co. that includes consulting or advisory, Bayer AG that includes consulting or advisory, and Merck that includes consulting or advisory. The other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The authors would like to thank Fatemeh Zaeimi, MSc, and Nastaran Shokri, BSc, for their assistance with the CTEPH database. This project received financial support from the Joint Department of Medical Imaging Academic Incentive Fund.
Figures


References
-
- Ende-Verhaar Y.M., Cannegieter S.C., Vonk Noordegraaf A., et al. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: a contemporary view of the published literature. Eur Respir J. 2017;49 - PubMed
-
- de Perrot M., Gopalan D., Jenkins D., et al. Evaluation and management of patients with chronic thromboembolic pulmonary hypertension - consensus statement from the ISHLT. J Heart Lung Transplant. 2021;40:1301–1326. - PubMed
-
- Madani M.M., Auger W.R., Pretorius V., et al. Pulmonary endarterectomy: recent changes in a single institution’s experience of more than 2,700 patients. Ann Thorac Surg. 2012;94:97–103. - PubMed
LinkOut - more resources
Full Text Sources
