

Exploration of the Interrelationship Between Serum Uric Acid, Gout, and Cardiac, Renal, and Metabolic Conditions in Middle Aged and Older People
- PMID: 40145269
- PMCID: PMC12132833
- DOI: 10.1161/JAHA.124.038723
Exploration of the Interrelationship Between Serum Uric Acid, Gout, and Cardiac, Renal, and Metabolic Conditions in Middle Aged and Older People
Abstract
Background: Cardiac, renal, and metabolic (CRM) conditions are major causes of morbidity and mortality globally. This study aims to explore the relationship between serum uric acid (SUA), hyperuricemia, gout, and CRM conditions in middle-aged and elderly populations.
Methods: Sample 1 included participants from CHARLS (China Health and Retirement Longitudinal Study, n=9341), and Sample 2 from NHANES (National Health and Nutrition Examination Survey, unweighted n=17 913; weighted n=115 646 390). Ordinal logistic regression, Cox regression, and restricted cubic spline analyses were used to assess the relationship between SUA, hyperuricemia, gout, and CRM conditions. A 2-sample Mendelian randomization analysis was conducted to explore causal associations between SUA and CRM conditions.
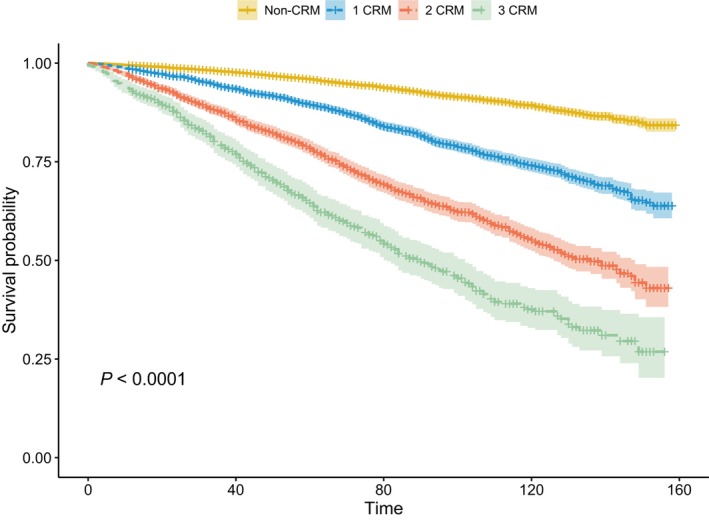
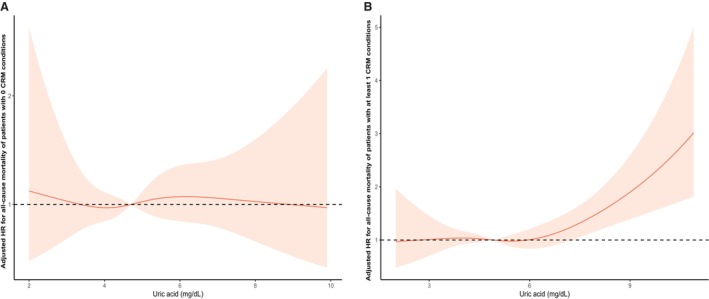
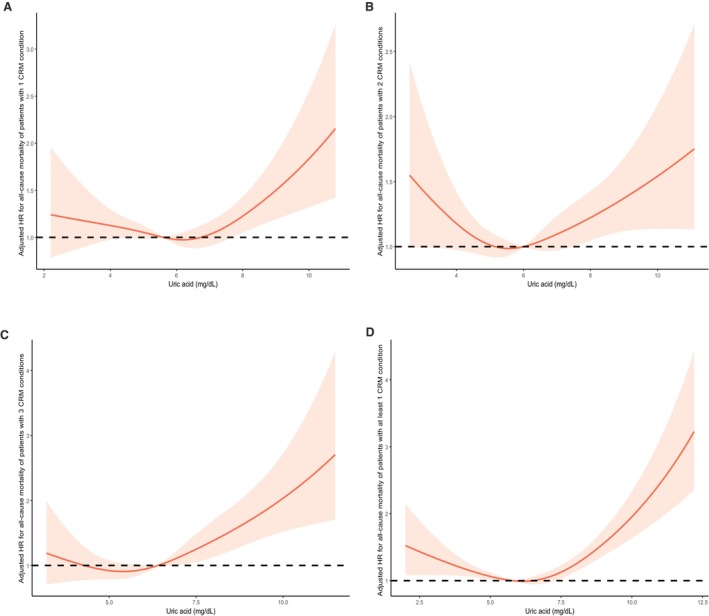
Results: In both samples, SUA, hyperuricemia, and gout were positively correlated with the risk of CRM conditions. Among participants with 3 or ≥1 CRM condition(s), SUA, asymptomatic hyperuricemia, and gout with poorly controlled hyperuricemia showed significant positive associations with all-cause mortality, whereas these associations were not observed in patients with gout with normal SUA levels. The restricted cubic spline analysis revealed a positive relationship between SUA levels and the risk of all-cause mortality in participants with ≥1 CRM condition(s), demonstrating a nonlinear dose-response relationship across both samples (P for nonlinearity <0.05). Mendelian randomization analysis indicated that SUA was causally associated with cardiovascular disease, chronic kidney disease, and diabetes.
Conclusions: Hyperuricemia and gout are strong predictors of increased prevalence and mortality of CRM conditions, emphasizing the importance of managing hyperuricemia and gout in these patients.
Keywords: Mendelian randomization; cardiac, renal, and metabolic conditions; gout; hyperuricemia; serum uric acid.
Conflict of interest statement
None.
Figures
References
-
- Ostrominski JW, Arnold SV, Butler J, Fonarow GC, Hirsch JS, Palli SR, Donato BMK, Parrinello CM, O'Connell T, Collins EB, et al. Prevalence and overlap of cardiac, renal, and metabolic conditions in US adults, 1999–2020. JAMA Cardiol. 2023;8:1050–1060. doi: 10.1001/jamacardio.2023.3241 - DOI - PMC - PubMed
-
- Ostrominski JW, Thierer J, Claggett BL, Miao ZM, Desai AS, Jhund PS, Kosiborod MN, Lam CSP, Inzucchi SE, Martinez FA, et al. Cardio‐renal‐metabolic overlap, outcomes, and Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. JACC Heart Fail. 2023;11:1491–1503. doi: 10.1016/j.jchf.2023.05.015 - DOI - PubMed
-
- Global burden of metabolic risk factors for chronic diseases C. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabetes Endocrinol. 2014;2:634–647. doi: 10.1016/S2213-8587(14)70102-0 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
