

IgG4-related ophthalmic disease presenting as posterior scleritis in a pediatric patient
- PMID: 40146480
- PMCID: PMC11950618
- DOI: 10.1186/s12348-025-00459-9
IgG4-related ophthalmic disease presenting as posterior scleritis in a pediatric patient
Abstract
Purpose: To report IgG4-related ophthalmic disease (IgG4-ROD) presenting as posterior scleritis in a pediatric patient.
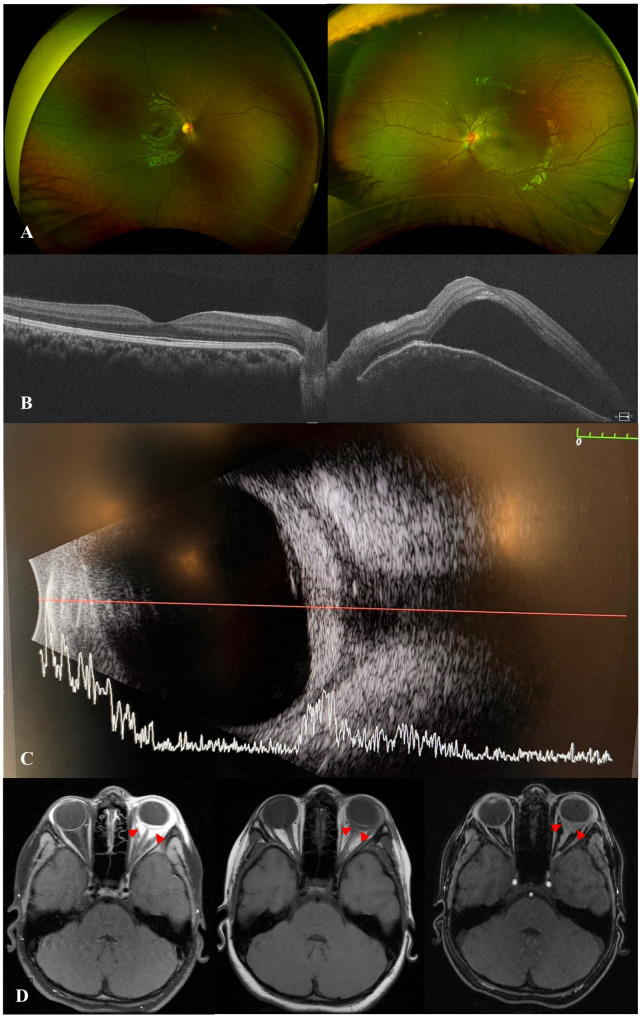
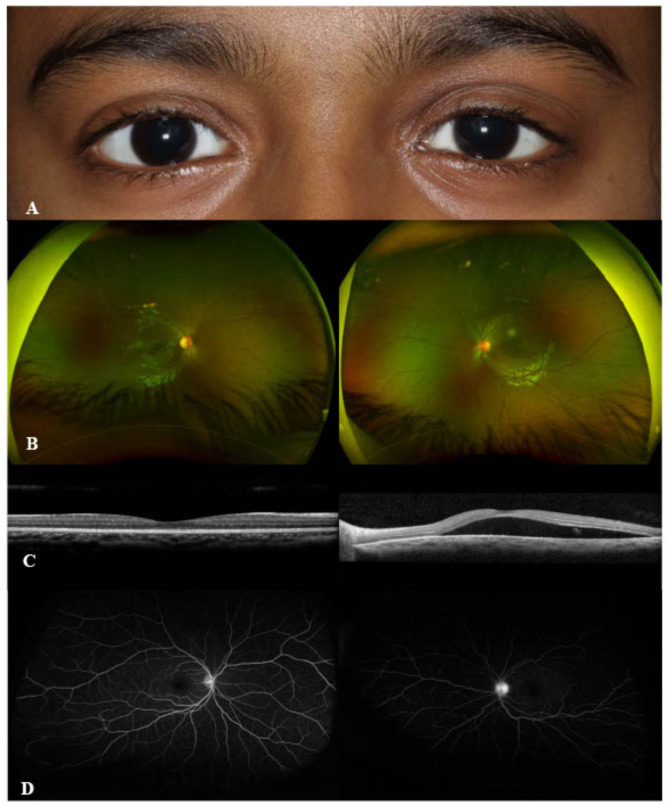
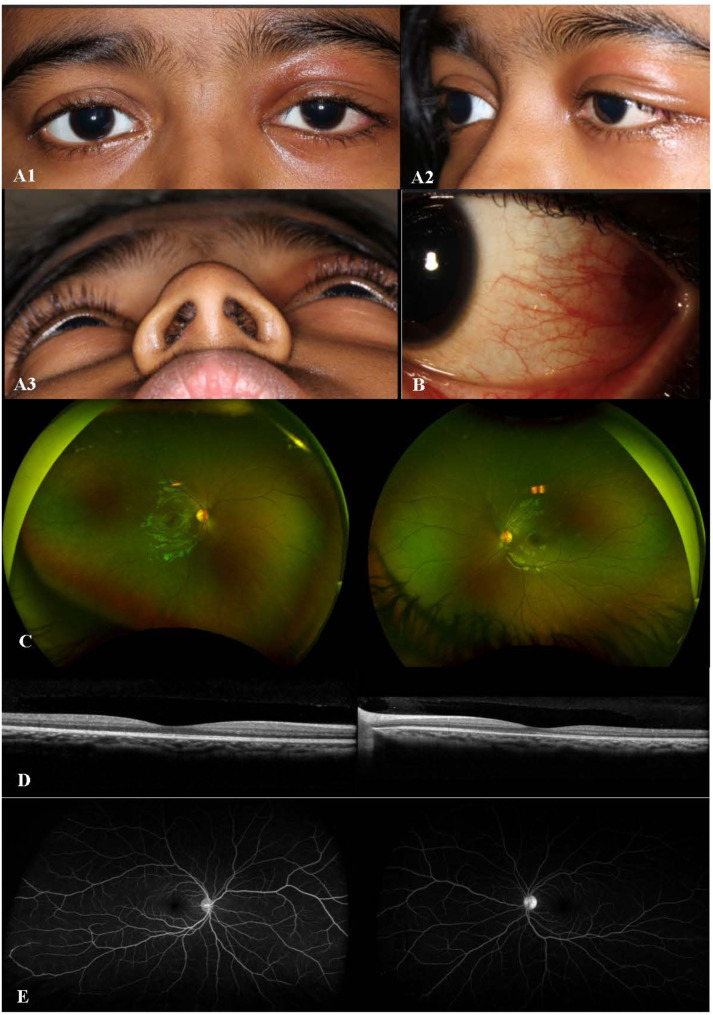
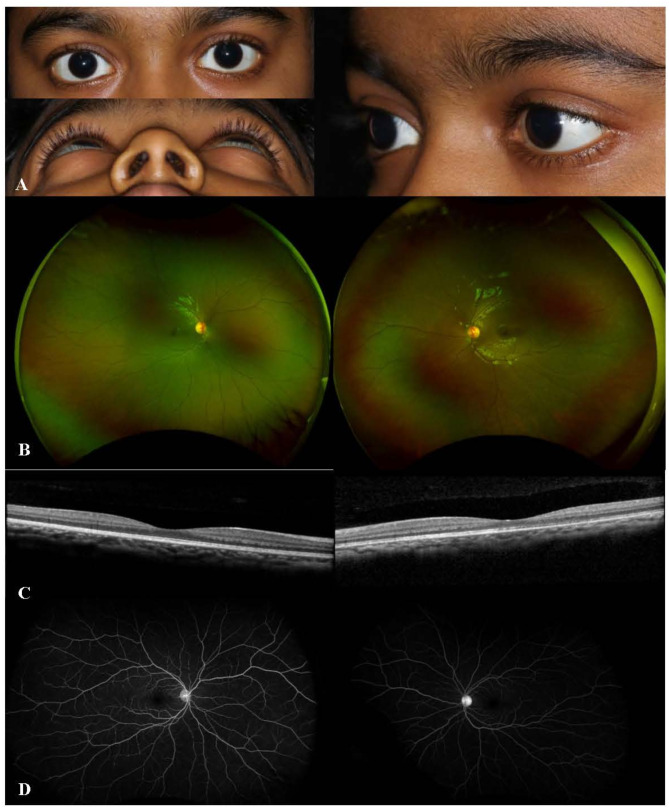
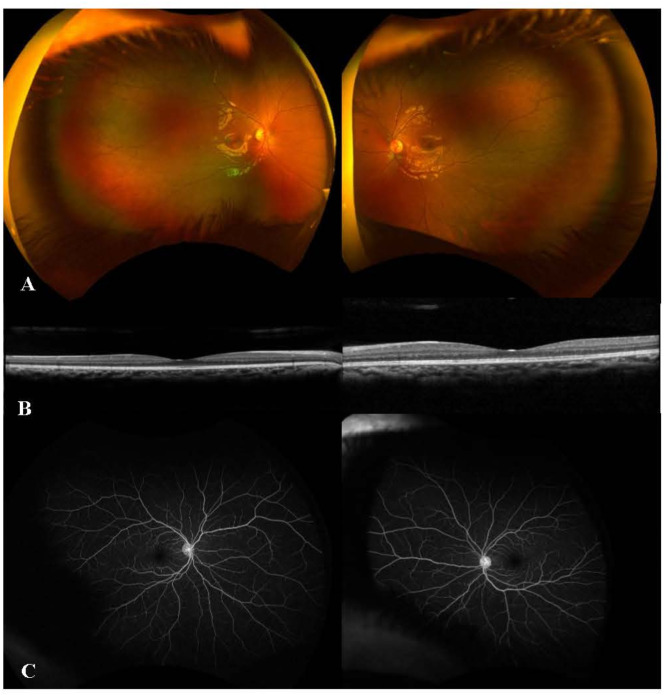
Observations: A 7-year-old girl presented with proptosis, painful eyelid swelling, and restricted extraocular movements (EOM) of her left eye (OS). Visual acuity (VA) was 20/20 in right eye (OD) and counting fingers (CF) at 1 foot in OS. Slit lamp examination revealed 2 + anterior chamber (AC) cells, optic disc edema (ODE) with elevated appearance of macula in OS. Optical coherence tomography (OCT) showed significant subretinal fluid (SRF) in macula, B-scan ultrasound (US) demonstrated T-sign in OS. Orbital MRI was also consistent with posterior scleritis and periorbital inflammation. Extensive systemic work-up was unremarkable. Thus, the patient was started on intravenous methylprednisolone (IVMP) 30 mg/kg/day for 3 days, along with topical therapy in OS, which led to an improvement of proptosis, EOM restriction, AC cells, as well as ODE and SRF in macula in OS. Fluorescein angiography (FA) showed leakage from optic disc in OS. The patient was then switched to oral prednisone with slow tapering and started on methotrexate (MTX). Given the recurrence of proptosis and painful eyelid swelling on systemic steroid tapering, serum IgG4 levels were ordered and found to be elevated at 149.9 mg/dL (range, 1-99). Therefore, the patient was diagnosed as 'possible' IgG4-ROD (based on diagnostic criteria) and started on infliximab (7.5 mg/kg) and IVMP monthly infusions with continuation of MTX 20 mg weekly and slower tapering of oral prednisone, which led to resolution of clinical findings, improvement of VA to 20/20 in OS.
Conclusion and importance: Posterior scleritis may be the initial presentation of IgG4-ROD in children. Refractory course is not uncommon. Biologics are effective in the long-term control of inflammation.
Keywords: IgG4-related ophthalmic disease; Infliximab; Pediatric; Posterior scleritis.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Ethics approval was obtained from The Stanford University Institutional Review Board, and informed consent was obtained from the patient’s parent. Consent for publication: Consent for publication was obtained from patient’s parent. Competing interests: The authors declare no competing interests. Meeting presentation: None.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
