

Controversies in treating nutcracker syndrome
- PMID: 40148589
- PMCID: PMC11950451
- DOI: 10.1186/s42155-025-00544-z
Controversies in treating nutcracker syndrome
Abstract
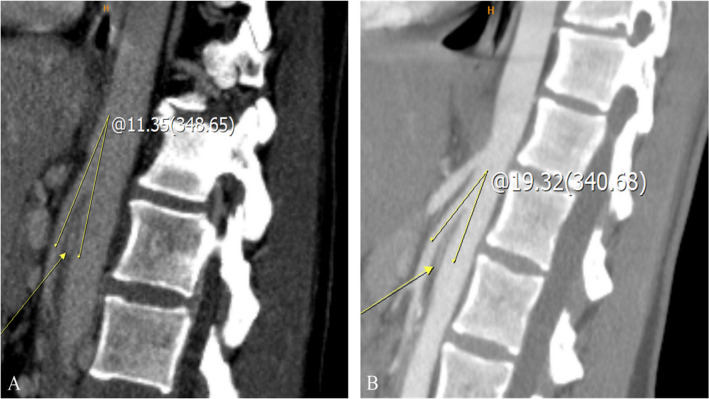
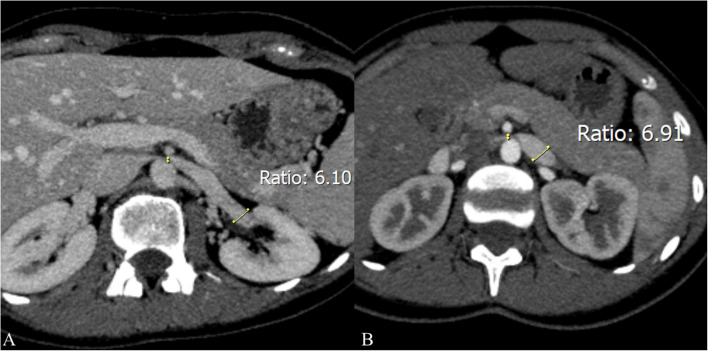
Nutcracker syndrome (NCS) is a relatively uncommon vascular condition characterized by compression of the left renal vein (LRV), resulting in a variable spectrum of nonspecific symptoms, including hematuria, flank pain, varicocele, and pelvic congestion syndrome. NCS can be classified into anterior and posterior types regarding the origin of LRV compression: anterior NCS occurs when LRV is compressed between the aorta and superior mesenteric artery, whereas posterior NCS involves LRV compression between the aorta and the spine. Despite advancements in diagnostic modalities, including Doppler ultrasound, computed tomography, magnetic resonance imaging, and invasive techniques like phlebography, there is still no globally accepted diagnostic algorithm, leading to inconsistencies in diagnosis. Moreover, due to the lack of standardized treatment guidelines, the optimal management of anterior NCS remains a topic of debate. While conservative management is usually recommended in the pediatric population, invasive treatments-including surgical options like LRV transposition and renal autotransplantation, as well as interventional radiology procedures like stenting, present challenges such as stent migration, restenosis, and long-term material durability. Nevertheless, the emergence of 3D-printed stents offers potential improvements in patient-specific treatment, particularly in the pediatric population, yet their clinical efficacy and safety remain under investigation. This brief communication addresses the current discussions regarding anterior NCS management, emphasizing the need for standardized diagnostic algorithms, a multidisciplinary approach, and continued technological advancements to refine treatment possibilities and strategies. Further research is critical to resolve these controversies and establish a consensus on best practices.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interest: Vi.Vi. is a member of the Editorial Board of CVIR Endovascular Journal; he did not participate in this article's selection or review processes. Other authors have no relevant financial or non-financial interests to disclose.
Figures




References
-
- Sablón González N, Lorenzo Villalba N, Parodis López Y, González Díaz P, Boada Díaz J, Kechida M. Síndrome del cascanueces [Nutcracker syndrome]. Medicina (B Aires). 2019;79:150–3. Spanish. - PubMed
-
- Quevedo HC, Arain SA, Abi RN. Systematic review of endovascular therapy for nutcracker syndrome and case presentation. Cardiovasc Revasc Med. 2014;15:305–7. 10.1016/j.carrev.2014.04.008. - PubMed
-
- Fong JK, Poh AC, Tan AG, Taneja R. Imaging findings and clinical features of abdominal vascular compression syndromes. AJR Am J Roentgenol. 2014;203:29–36. 10.2214/AJR.13.11598. - PubMed
LinkOut - more resources
Full Text Sources