

Concurrent robotic colorectal surgical oncology training within a structured mentored international fellowship program
- PMID: 40148715
- PMCID: PMC11950044
- DOI: 10.1007/s11701-025-02287-4
Concurrent robotic colorectal surgical oncology training within a structured mentored international fellowship program
Abstract
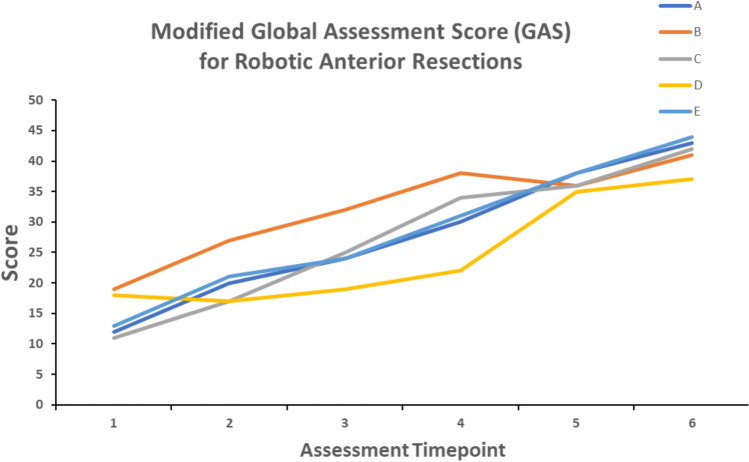
Robotic colorectal surgery is increasingly adopted worldwide, with mentored programs for established surgeons becoming more common. However, there is a paucity of dedicated robotic training programs for colorectal fellows. This study aims to assess the feasibility and efficacy of a structured, apprentice-based robotic colorectal training program delivered to multiple fellows concurrently. The fellowship program incorporates simulation training, dry/wet laboratory work, dedicated robotic console time in the operating room (OR) and individualised mentorship. Overall robotic proficiency was assessed using the Global Evaluative Assessment of Robotic Skills (GEARS) and procedure-specific proficiency was assessed using a modified European Academy of Robotic Colorectal Surgery (EARCS) Global Assessment Score (GAS) throughout the fellowship. A total of 59 cases (29 right hemicolectomies, 30 anterior resections) were evaluated between August 2023 and July 2024. Significant improvements were observed in GEARS scores (p = 0.0065) and modified GAS for both right hemicolectomies (p = 0.0052) and anterior resections (p = 0.0005), demonstrating a high level of competence and independence. Mean operative times were 213 min (right hemicolectomy) and 328 min (anterior resection). Median length of stay in the hospital was 2 days (right hemicolectomy) and 4 days (anterior resection). Median lymph node yield was 29 (right hemicolectomy) and 26 (anterior resection). There was 0% involved margins for both procedures. Robotic colorectal surgical oncology training delivered to multiple fellows concurrently in an apprenticeship model with dedicated console time is achievable and successful, leading to high levels of robotic competency and independence, whilst maintaining a high standard of clinical care and oncological outcome.
Keywords: Fellowship; Robotic colorectal surgery; Training.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Conflict of interest: The authors declare no competing interests. Ethical statement: This is an observational study. Ethical approval was waivered by the Memorial Sloan Kettering Cancer Center (MSKCC) institutional board.
Figures


References
-
- Feng Q, Yuan W, Li T, Tang B, Jia B, Zhou Y et al (2022) Robotic versus laparoscopic surgery for middle and low rectal cancer (REAL): short-term outcomes of a multicentre randomised controlled trial. Lancet Gastroenterol Hepatol 7(11):991–1004 - PubMed
-
- Park JS, Lee SM, Choi GS, Park SY, Kim HJ, Song SH et al (2023) Comparison of laparoscopic versus robot-assisted surgery for rectal cancers: The COLRAR Randomized Controlled Trial. Ann Surg 278(1):31–38 - PubMed
-
- Harji D, Houston F, Burke J, Griffiths B, Tilney H, Miskovic D et al (2023) The current status of robotic colorectal surgery training programmes. J Robot Surg 17(2):251–263 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
