

The mechanisms and applications of endothelial progenitor cell therapy in the treatment of intracranial aneurysm
- PMID: 40148864
- PMCID: PMC11951544
- DOI: 10.1186/s12967-025-06401-w
The mechanisms and applications of endothelial progenitor cell therapy in the treatment of intracranial aneurysm
Abstract
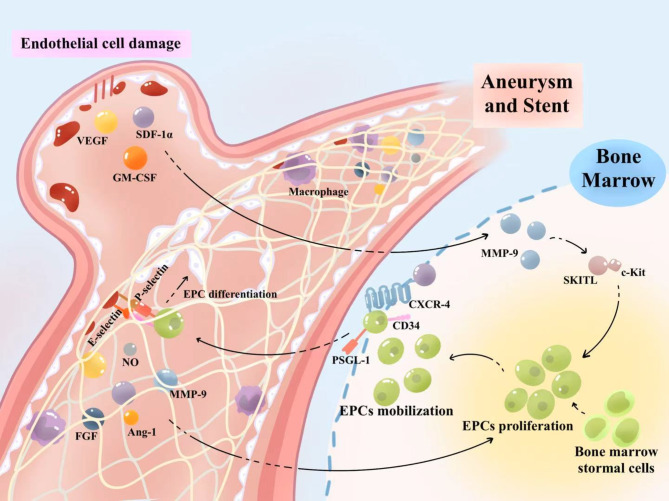
The pathophysiological mechanism of intracranial aneurysm (IA) involves the dynamic interaction of ECM abnormalities, hemodynamic stress, and inflammatory response. The rupture of intracranial aneurysm will cause serious consequences. Multiple studies have confirmed the important role and potential application of endothelial progenitor cells (EPCs) in vascular repair. This review focuses on the specific mechanism of EPCs in the treatment of intracranial aneurysms, which promote re-endothelialization and angiogenesis through bone marrow mobilization, targeted migration to the site of injury, differentiation into mature endothelial cells, and secretion of angiogenic factors. In addition, EPCs maintain ECM homeostasis by regulating MMP/IMP balance, inhibiting aneurysm wall thinning and structural damage. Based on the vascular repair mechanism of EPCs, new treatment strategies such as "biologically active" spring coils (loaded with EPCs or SDF-1α) and flow diverters(FDs) combined with EPCs therapy have been developed to synergistically promote carotid endothelialization of aneurysms and reduce the risk of recurrence. Future research needs to further validate the long-term efficacy and precise regulatory mechanisms of EPCs in clinical translation, providing new directions for IA treatment.
Keywords: Endothelial progenitor cell; Endothelialization; Endovascular treatment; Intracranial aneurysm.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: No applicable. Consent for publication: Not applicable. Competing interests: The authors declare that they have no competing interests.
Figures

References
-
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol Jul. 2011;10(7):626–36. - PubMed
-
- Brown RD Jr., Broderick JP. Unruptured intracranial aneurysms: epidemiology, natural history, management options, and Familial screening. Lancet Neurol Apr. 2014;13(4):393–404. - PubMed
-
- Tawk RG, Hasan TF, D’Souza CE, Peel JB, Freeman WD. Jul. Diagnosis and Treatment of Unruptured Intracranial Aneurysms and Aneurysmal Subarachnoid Hemorrhage. Mayo Clin Proc. 2021;96(7):1970–2000. - PubMed
-
- Brisman JL, Song JK, Newell DW. Cerebral aneurysms. N Engl J Med Aug. 2006;31(9):928–39. - PubMed
Publication types
MeSH terms
Grants and funding
- 23Y1404500/Shanghai Sailing Program
- 82171311/National Natural Science Foundation of China
- 82330039/National Natural Science Foundation of China
- 82271339/National Natural Science Foundation of China
- 82301489/National Natural Science Foundation of China
- 82201462/National Natural Science Foundation of China
- 21XD1400600/Shanghai Excellent Academic Leader Program
- 20224Y0072/Special Clinical Research Project in Health Industry of Shanghai Municipal Health Commission
- SHDC2020CR2034B/Clinical Research Plan of SHDC
- 2022ZZ01006/Shanghai Municipal Health Commission
- GWVI-11.1-17/Shanghai Municipal Health Commission
LinkOut - more resources
Full Text Sources
Medical
