

Combinatory Flowcytometric Approach in Pediatric Acute Lymphoid Leukemia Identifies Surrogate Minimal Residual Disease Markers
- PMID: 40150002
- PMCID: PMC11941652
- DOI: 10.3390/diagnostics15060658
Combinatory Flowcytometric Approach in Pediatric Acute Lymphoid Leukemia Identifies Surrogate Minimal Residual Disease Markers
Abstract
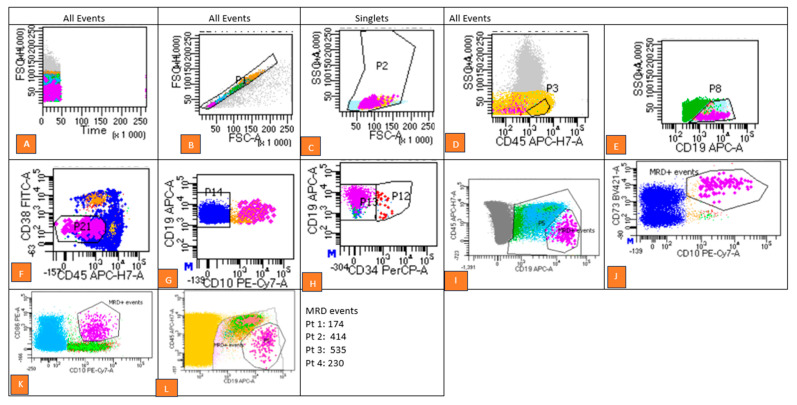
Background/Objectives: Minimal residual disease (MRD) refers to the resistant clonal population of leukemia cells that survive induction chemotherapy, serving as a critical indicator of treatment response in pediatric Acute Lymphoid Leukemia (ALL). While flow cytometry (FCM) and molecular methods are standard for MRD detection, novel leukemia-associated immunophenotype (LAIP) markers are needed when conventional markers are insufficient. Methods: MRD was assessed in 218 pediatric B-ALL patients using a combinatory approach of Different-from-Normal (DfN) and LAIP strategies. An eight-color flow cytometry panel included routine MRD markers (e.g., CD10, CD19, and CD20) and less commonly used markers (e.g., CD123, CD73, CD86). Cytogenetic and molecular profiling were integrated to evaluate the association between genetic abnormalities and MRD positivity. Results: The combined DfN and LAIP approach enhanced MRD detection sensitivity compared to individual methods. CD7 showed a significant association with MRD positivity (p = 0.003), whereas CD73 (p = 0.000) and CD86 (p = 0.002) correlated with MRD-negative status. CD123 exhibited the highest aberrancy among MRD-positive cases, while CD81 had the lowest. These findings highlight the prognostic potential of CD73 and CD86 for MRD-negative status, complementing the established utility of CD123. Conclusions: Incorporating novel markers (CD123, CD73, CD86, and CD81) into MRD panels enhances detection sensitivity and clinical applicability. These markers are compatible with standard flow cytometry, supporting their integration into routine practice for comprehensive MRD evaluation, ultimately improving therapeutic outcomes in pediatric B-ALL.
Keywords: DfN; LAIP; acute leukemia; flow cytometry; minimal residual disease (MRD).
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Evaluation of new markers for minimal residual disease monitoring in B-cell precursor acute lymphoblastic leukemia: CD73 and CD86 are the most relevant new markers to increase the efficacy of MRD 2016; 00B: 000-000.Cytometry B Clin Cytom. 2018 Jan;94(1):100-111. doi: 10.1002/cyto.b.21486. Epub 2016 Oct 27. Cytometry B Clin Cytom. 2018. PMID: 27718302
-
The Evolving Landscape of Flowcytometric Minimal Residual Disease Monitoring in B-Cell Precursor Acute Lymphoblastic Leukemia.Int J Mol Sci. 2024 Apr 30;25(9):4881. doi: 10.3390/ijms25094881. Int J Mol Sci. 2024. PMID: 38732101 Free PMC article. Review.
-
[Minimal residual disease monitoring by flow cytometry in children with acute lymphoblastic leukemia].Klin Lab Diagn. 2010 Aug;(8):36-41. Klin Lab Diagn. 2010. PMID: 20886718 Russian.
-
Faster clinical decisions in B-cell acute lymphoblastic leukaemia: A single flow cytometric 12-colour tube improves diagnosis and minimal residual disease follow-up.Br J Haematol. 2024 May;204(5):1872-1881. doi: 10.1111/bjh.19390. Epub 2024 Mar 3. Br J Haematol. 2024. PMID: 38432068
-
Minimal residual disease detection using flow cytometry: Applications in acute leukemia.Med J Armed Forces India. 2016 Apr;72(2):152-6. doi: 10.1016/j.mjafi.2016.02.002. Epub 2016 Mar 29. Med J Armed Forces India. 2016. PMID: 27257325 Free PMC article. Review.
References
-
- Willemse M.J., Seriu T., Hettinger K., d’Aniello E., Hop W.C., Panzer-Grümayer E.R., Biondi A., Schrappe M., Kamps W.A., Masera G., et al. Detection of Minimal Residual Disease Identifies Differences in Treatment Response between T-All and Precursor B-All. Blood. 2002;99:4386–4393. doi: 10.1182/blood.V99.12.4386. - DOI - PubMed
-
- Brisco M.J., Condon J., Hughes E., Neoh S.H., Sykes P.J., Seshadri R., Toogood I., Waters K., Tauro G., Ekert H., et al. Outcome prediction in childhood acute lymphoblastic leukaemia by molecular quantification of residual disease at the end of induction. Lancet. 1994;343:196–200. doi: 10.1016/S0140-6736(94)90988-1. - DOI - PubMed
-
- Seth N., Mahajan V., Kedia S., Sutar A., Sehgal K. Minimal Residual Disease (MRD) detection in B- ALL—Experience of a standalone flow cytometry laboratory. Pediatr. Hematol. Oncol. J. 2021;6:26–31. doi: 10.1016/j.phoj.2020.12.003. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
